Abstracts
OBJECTIVE: To analyze the characteristics of visits to the emergency services that result from falls and to identify the factors associated with these visits. METHOD: A cross-sectional study of 12,617 visits that resulted from falls, recorded in the National Injury Surveillance System, was carried out. The data were collected in 23 Brazilian capitals and the Federal District between September and November 2009 using cluster sampling. Correspondence analysis was used, which allowed for the joint observation of a large number of qualitative variables. RESULTS: Most of the victims were male (56.5%), aged 0 to 19 years (45.7%), and identified as non-white skin color (62.2%). The majority of the falls occurred at home (54.6%) and in the street (17.4%); 14.3% were work-related. The predominant types were "falls on the same level" (57.0%) and "falls from a ladder/step" (15.6%). Most of the injuries were classified as sprains, dislocations, bruises, cuts, or lacerations (68.3%). Falls among children occurred mostly at home; among adolescents at school; and among young people at sports facilities. Falls among adults were associated with the work place, including falls from scaffolding, roofs, stairs/steps, and holes and were linked to alcohol use. Falls on the same level resulted in less serious injuries, mostly on the upper and lower limbs, and falls from scaffolding and roofs were associated with more severe injuries and hospitalization. CONCLUSIONS: The results show that strategies to prevent falls should target residences, schools, and work environments.
External Causes; Accidental Falls; Emergency Medical Services; Risk Factors; Cross-Sectional Studies
OBJETIVO: Analisar as características dos atendimentos decorrentes de quedas em serviços de urgência e emergência e identificar fatores associados. MÉTODOS: Estudo transversal com 12.617 atendimentos decorrentes de quedas registrados no Sistema de Vigilância de Violências e Acidentes, coletados em 23 capitais e Distrito Federal, de setembro a novembro de 2009, por meio de uma amostra por conglomerado. Foi utilizada a técnica de análise de correspondência, por permitir a observação conjunta de um grande número de variáveis qualitativas. RESULTADOS: A maior parte das vítimas foi do sexo masculino (56,5%), faixa etária de 0 a 19 anos (45,7%) e declarados não brancos (62,2%). A maioria das quedas ocorreu na residência (54,6%) e via pública (17,4%); 14,3% foram relacionadas ao trabalho. Os tipos predominantes foram "queda no mesmo nível" (57,0%) e "queda de escada/degrau" (15,6%). A maioria das lesões foi classificada como entorse, luxação, contusão, corte e laceração (68,3%). Quedas dentre as crianças associaram-se à ocorrência na residência; com os adolescentes na escola; e jovens na prática esportiva. Quedas em adultos estiveram associadas ao local de trabalho, queda de andaimes, telhados, escada/degrau e buracos e uso de álcool. As quedas no mesmo nível resultaram em lesões de menor gravidade, em membros inferiores e superiores, e as quedas de andaime e telhado se associaram com lesões de maior gravidade e internações. CONCLUSÕES: Os resultados mostram que estratégias para a prevenção das quedas devem ser implantadas particularmente em residências, escolas e ambientes de trabalho.
Causas externas; Acidentes por Quedas; Serviços Médicos de Emergência; Fatores de Risco; Estudos Transversais
OBJETIVO: Objetivo: Analizar las características de las atenciones realizadas por caídas en servicios de urgencia y emergencia e identificar factores asociados. MÉTODOS: Estudio transversal con 12.617 atenciones realizadas por caídas registradas en el Sistema de Vigilancia de Violencias y Accidentes, colectadas en 23 Capitales y Distrito Federal de Brasil, de septiembre a noviembre de 2009 por medio de una muestra por conglomerado. Se utilizó la técnica de análisis de correspondencia, por permitir un análisis conjunto de un gran número de variables cualitativas. RESULTADOS: La mayor parte de las víctimas fue del sexo masculino (56,5%), grupo de 0 a 19 años (45,7%) y declarados no blancos (62,2%). La mayoría de las caídas ocurrió en la residencia (54,6%) y vía pública (17,4%); 14,3% fueron relacionadas con el trabajo. Los tipos predominantes fueron "caída en el mismo nivel" (57,0%) y "caída de escalera/escalón" (15,6%). La mayoría de las lesiones fue clasificada como esguince, luxación, contusión, corte y laceración (68,3%). Caídas entre los niños se asociaron con la residencia, en los adolescentes con la escuela, y en jóvenes con la práctica deportiva. Caídas en adultos estuvieron asociadas con el lugar de trabajo, caída de andamios, tejados, escalera/escalón y huecos y uso de alcohol. Las caídas en el mismo nivel resultaron en lesiones de menor gravedad, en miembros inferiores y superiores y las caídas de andamio y tejado se asociaron con lesiones de mayor gravedad e internaciones. CONCLUSIONES: Los resultados muestran que estrategias para la prevención de las caídas deben ser implantadas particularmente en residencias, escuelas y ambientes de trabajo.
Causas Externas; Accidentes por Caídas; Servicios Médicos de Urgencia; Factores de Riesgo; Estudios Transversales
ORIGINAL ARTICLES
Deborah Carvalho MaltaI; Marta Maria Alves da SilvaI; Márcio Dênis Medeiros MascarenhasII; Naíza Nayla Bandeira de SáI; Otaliba Libânio de Morais NetoI; Regina Tomie Ivata BernalIII; Rosane Aparecida MonteiroIV; Silvânia Suely Caribé de Araújo AndradeI; Vilma Pinheiro GawryszewskiV, VI
IDepartamento de Análise de Situação de Saúde. Secretaria de Vigilância em Saúde. Ministério da Saúde. Brasília, DF, Brasil
IIHospital Universitário. Universidade Federal do Piauí. Teresina, PI, Brasil
IIIFaculdade de Saúde Pública. Universidade de São Paulo. São Paulo, SP, Brasil
IVDepartamento de Medicina Social. Faculdade de Medicina de Ribeirão Preto. Universidade de São Paulo. São Paulo, SP, Brasil
VCentro de Vigilância Epidemiológica. Secretaria de Estado da Saúde de São Paulo. São Paulo, SP, Brasil
VIHealth Analysis & Information. Pan American Health Organization. Washington, DC, United States
Correspondence
ABSTRACT
OBJECTIVE: To analyze the characteristics of visits to the emergency services that result from falls and to identify the factors associated with these visits.
METHOD: A cross-sectional study of 12,617 visits that resulted from falls, recorded in the National Injury Surveillance System, was carried out. The data were collected in 23 Brazilian capitals and the Federal District between September and November 2009 using cluster sampling. Correspondence analysis was used, which allowed for the joint observation of a large number of qualitative variables.
RESULTS: Most of the victims were male (56.5%), aged 0 to 19 years (45.7%), and identified as non-white skin color (62.2%). The majority of the falls occurred at home (54.6%) and in the street (17.4%); 14.3% were work-related. The predominant types were "falls on the same level" (57.0%) and "falls from a ladder/step" (15.6%). Most of the injuries were classified as sprains, dislocations, bruises, cuts, or lacerations (68.3%). Falls among children occurred mostly at home; among adolescents at school; and among young people at sports facilities. Falls among adults were associated with the work place, including falls from scaffolding, roofs, stairs/steps, and holes and were linked to alcohol use. Falls on the same level resulted in less serious injuries, mostly on the upper and lower limbs, and falls from scaffolding and roofs were associated with more severe injuries and hospitalization.
CONCLUSIONS: The results show that strategies to prevent falls should target residences, schools, and work environments.
Descriptors: External Causes. Accidental Falls. Emergency Medical Services. Risk Factors. Cross-Sectional Studies.
RESUMEN
OBJETIVO: Objetivo: Analizar las características de las atenciones realizadas por caídas en servicios de urgencia y emergencia e identificar factores asociados.
MÉTODOS: Estudio transversal con 12.617 atenciones realizadas por caídas registradas en el Sistema de Vigilancia de Violencias y Accidentes, colectadas en 23 Capitales y Distrito Federal de Brasil, de septiembre a noviembre de 2009 por medio de una muestra por conglomerado. Se utilizó la técnica de análisis de correspondencia, por permitir un análisis conjunto de un gran número de variables cualitativas.
RESULTADOS: La mayor parte de las víctimas fue del sexo masculino (56,5%), grupo de 0 a 19 años (45,7%) y declarados no blancos (62,2%). La mayoría de las caídas ocurrió en la residencia (54,6%) y vía pública (17,4%); 14,3% fueron relacionadas con el trabajo. Los tipos predominantes fueron "caída en el mismo nivel" (57,0%) y "caída de escalera/escalón" (15,6%). La mayoría de las lesiones fue clasificada como esguince, luxación, contusión, corte y laceración (68,3%). Caídas entre los niños se asociaron con la residencia, en los adolescentes con la escuela, y en jóvenes con la práctica deportiva. Caídas en adultos estuvieron asociadas con el lugar de trabajo, caída de andamios, tejados, escalera/escalón y huecos y uso de alcohol. Las caídas en el mismo nivel resultaron en lesiones de menor gravedad, en miembros inferiores y superiores y las caídas de andamio y tejado se asociaron con lesiones de mayor gravedad e internaciones.
CONCLUSIONES: Los resultados muestran que estrategias para la prevención de las caídas deben ser implantadas particularmente en residencias, escuelas y ambientes de trabajo.
Descriptores: Causas Externas. Accidentes por Caídas. Servicios Médicos de Urgencia. Factores de Riesgo. Estudios Transversales.
Introduction
Many people experience unintentional falls. Falls affect people of all ages, genders, and socioeconomic conditions. Some groups have a greater likelihood of suffering from a fall, such as children, the elderly,3,13 workers,15 and athletes.6 Falls occur in various locations, including the home, public areas, school, the work place, and leisure areas.
The impact of falls on individual health varies greatly. One fall may result in no injury, but another may lead to injuries of various degrees of severity, disability, time off from work, and even death. For example, studies show that these events can seriously affect quality of life for the elderly and that the fear of falling may restrict people's activities and mobility, decrease physical activity, and cause social isolation and depression.3,13
Due to the high frequency of falls, this issue deserves attention in public health as one of the leading causes of mortality worldwide. Estimates from the U.S. show that falls are the principal cause of non-fatal injuries for children and adolescents under 19, and that approximately 2.8 million childrenª and 1.7 million people over 651 are treated annually in U.S. emergency services due to falls.
In Brazil, falls affect the national mortality rate and have an even greater impact on morbidity, according to official sources of health information. Data from the Mortality Information System (Sistema de Informações sobre Mortalidade, or SIM) show that 9,171 deaths resulted from falls in 2009, which represents 6.6% of total deaths due to external causes.
Unintentional falls result from a variety of risk factors, and it is difficult to identify a single causal factor in the event of a fall. However, preventative programs and measures may reduce a considerable number of falls. Therefore, it is essential to increase awareness about the dangers of falls and their characteristics, consequences, and risk factors. Studies using data from emergency services are particularly appropriate for this purpose because they provide detailed information about the victims, circumstances, and locations of falls, which are not provided in official mortality and morbidity data. This study aims to describe the characteristics of emergency service visits that result from falls and identify the associated factors.
Method
The analyzed data include 12,617 visits resulting from falls in 2009 and are available in VIVA's database of external causes. The methodology for these data has been presented in other publications.9,
VIVA's 2009 survey component is a cross-sectional study. The data were collected every 12 hours over 30 consecutive days from September to November 2009. We chose different emergency services in the Brazilian Unified Health System (SUS) using probability. The study population consisted of the victims of violence and accidents (external causes) who sought emergency treatment in the selected municipalities.
Academics in nursing and medicine and healthcare professionals conducted the interviews under the supervision of technicians from Health Departments. The collected data were recorded in proper form. We ensured that our collection procedures were standardized by training technicians from the state and municipal health departments, which are overseen by the Health Surveillance Secretary (Secretaria de Vigilância em Saúde, SVS) and the Surveillance Coordination for Non-communicable Diseases and Injuries (Coordenação de Vigilância de Doenças e Agravos Não Transmissíveis da Secretaria). The data were entered into the software EpiInfo 3.5.1 for each participating municipality's Department of Epidemiological Surveillance. The technical staff from the Ministry of Health examined the consistency of the data using Link Plus software, version 2.0.
The research project included 74 emergency service centers in the Federal District and 23 Brazilian state capitals. The centers were selected based on the criteria of the availability of services for injuries due to external causes, accreditation and registration in the National Register of Health Facilities (Cadastro Nacional de Estabelecimentos de Saúde, CNES), number of visits, range of services provided, and treatment success. Additionally, the project considered how each health department's technical staff viewed their emergency care services. We estimated our sample size using the number of visits for injuries due to external causes, recorded in the Hospital Information System (SIH/SUS), and the proportion of visits from VIVA's 2006-2007 research project. Furthermore, we used accuracy criteria for our study's estimates. Based on these criteria (coefficient of variation below 30% and standard error below three), the sample size included at least 750 visits for injuries due to external causes in the Federal District and 1,500 in the state capitals.
Based on previous studies and the large volume of cases treated in these centers, we decided to conduct a sample of all the cases. To do so, we used single-state cluster sampling.7,16 The primary sampling unit (UPA) consisted of 12-hour shifts in centers that were selected in each municipality. To randomly select shifts, we assigned two shifts per day to the 30-day collection period for a total of 60 shifts. To define the number of shifts sampled in each facility, we used a ratio of the minimum sample size of primary care visits (2009) for injuries due to external causes and the average number of such visits to the same institution in previous years. To ensure a minimum sample size in the capitals, we randomly sampled two extra shifts.
The following variables were examined: 1) demographics (gender, age, race, and education); 2) event characteristics (type of violence, victim/aggressor relationship, location of occurrence, repeat offense); and 3) referrals to the service network (i.e., referrals to other institutions outside the healthcare sector). To improve our interpretation of the results, we used correspondence analysis, which is an appropriate technique for qualitative variables. Correspondence analysis is equivalent to factor analysis, and the results are presented graphically. The smallest distances between the rows and columns represent the strongest association between the categories, and a greater distance represents disassociation.14 The correspondence analysis11 applies mainly to contingency tables, where the rows and columns in the table are dependent on each other. It is also useful for a large number of variables because it allows for a joint, exploratory analysis and summarizes the variability of the data in few dimensions. This analysis was performed using the SPSS software version 13.0.
The algorithm for correspondence analysis that is available in statistical software assumes that the data come from single random sampling. However, Souza et al17 warned that using this technique on data from complex sampling planes, without considering this source, affects the quality of the results. We considered the sample weights to calculate the proportions of each cell in the table so that the resulting graph will reflect the population proportions. In this context, we first produced the expanded contingency tables (total visits) and, from them, developed the correspondence graph.
The estimator18 for total visits to emergency services due to accidents and violence in the 30-day period is given by the equation:

where:
whij is the sample weight in the h-th stratum (CNES); i-th is the UPA (shift); and j-th is the number of elements in the h-th stratum of i-th UPA.
yhij is the value observed for the variable (1 if it was observed and 0 if not) in the h-th stratum, the i-th UPA, and the j-th number of elements in the h-th stratum of i-th UPA.
The National Commission of Ethics in Research approved the research project (Opinion nº 439/2009, 07/21/2011). Because this study examines national epidemiologic surveillance, we replaced verbal consent from the patient or guardian with a consent form, which was recorded in a proper form. We guaranteed total anonymity and privacy to the patients, professionals, and service managers and the freedom to cease participation in the interview at any time without repercussions for the participant or family, in accordance with Resolution 196/1996.
RESULTS
The data presented below refer to the 12,617 visits due to falls that were registered by VIVA during the 2009 survey. These visits represented between 30.7% and 32.3% of the cases treated during the studied 30-day period in the 74 emergency service centers we sampled in 23 capitals and the Federal District.
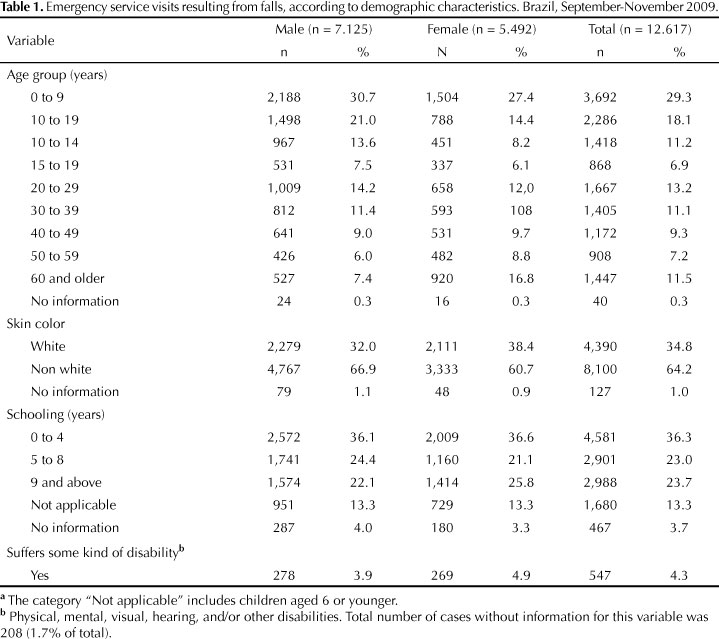
Table 1 shows the predominance of male patients, who represented 56.5% of visits. Regarding age, the highest rates were observed among children and adolescents, followed by young adults and the elderly. The 0-9 age group represented 29.3% of the total visits; 10-19-years, 18.1%; 20-29 years, 13.2%; and 60 years and above, 11.5%. These age groups were the most frequent for both females and males. Regarding race, non-white individuals represented 64.2% of the victims (8,100/12,617). We observed that approximately 65.2% of the falls among males were suffered by non-white males (4,767/7,125) and that 58.3% (3,333/5,492) of the falls among females were suffered by non-white women. The largest proportion of the cases aged six or above and with no serious mental disability on record had up to four years of education (36.3%). They were followed by patients who had at least nine years of formal education (23.7%) and those with four to eight years of formal education (23.0%). The distribution of the variable by gender showed no significant differences. A total of 4.3% of the sample, with 4.9% of women and 3.9% of men, reported some type of disability (physical, mental, visual, auditory, and/or other disabilities).
Table 2 shows the characteristics of the events: 13.5% of all visits were work-related falls (16.2% for males and 10.0% for females). Alcohol consumption in the six hours prior to the fall, as reported by the victim, had occurred in 6.3% of the cases, with men reporting a rate 4.1 times higher than that of females (8.9% and 2.8%, respectively). Notably, if we include the service visits for which the interviewer suspected unreported alcohol use, this proportion reaches 11.4% (data not shown).
More than half of the falls (55.9%) occurred at home, followed by the street (16.4%). The proportion of women who suffered falls at home was greater than that of men (64.8% and 49.1%, respectively). The most frequent type of fall occurred on the same level (55.2%), followed by a fall from a step (14.6%). Mild lesions were the most common form of injury: sprains and strains (26.2%), bruises (23.7%), and cuts/lacerations (19.0%). However, 16.8% of the falls resulted in fractures, and 3.9% resulted in traumatic brain injury. Injuries mainly occurred on the upper limbs (29.2%), lower limbs (27.0%), and the head/face (26.1%). The most frequent types of injuries and injury location were the same for women and men. After the emergency response, 79.4% of patients were discharged; 7.1% were hospitalized.
The correspondence analysis showed that two dimensions (sets of associated variables) explained 81% of the total variation; the first explained 52%, and the second explained 29%. Thus, we concluded that there is an association between certain demographic variables and certain characteristics of falls. Dimension 1 consists of the age categories zero to nine years (35%), 20 to 39 years (21%); victims with at least nine years of schooling (11%); and the categories of alcohol (16%), trade/service (15%), residence (12%), and industry/construction (6%). Dimension 2 comprises the age categories of 10 to 14 years, 15 to 19 years, and 60 and above, which contributed 61% of the total, and the categories school and sports facility (67%).
These associations can be better observed when they are represented graphically. Figure 1 shows the association (proximity between points) between demographic variables (age, gender, and schooling), disability, alcohol use reported by the victim, place of fall, and type of fall. This figure brings together the variables that showed an association. This technique helped us to visualize the associations between the low-frequency variables, which cannot be adequately observed with other techniques. Figure 1 shows five groups. The first group shows that falls are associated with sports facilities for adolescents and youth between the ages of 15 and 19. The second group shows an association between children in the 10 to 14 age range, falls from trees, and the location of school. The third group shows that accidents among adults aged 20 to 59 are associated with the workplace (industry/construction and commerce/service), alcohol consumption, and falls from scaffolding, the roof, ladders/steps, and into holes. The fourth group shows an association between reported disabilities and falls among people aged 60 and above. Finally, the fifth group shows associations between falls among children aged 0-9, home residence, falls from the bed and other furniture, 0-4 years of schooling, and female gender.
Figure 2 shows the associations between type of fall, type of injury, location of injury, and treatment at the emergency room. Two groups summarize the observed associations between the variables. The events that led to discharge or hospitalization are different in these opposing groups. The group on the right shows that falls on the same level are associated with less serious injuries, such as sprains and bruises on the upper and lower limbs, and resulted in hospital discharge within 24 hours. The group on the left shows associations between falls from scaffolding and roofs and more serious injuries, such as multiple traumas, injuries to multiple organs, fractures, and intracranial injuries, which caused the victims to be hospitalized or referred to out-patient units and other services.
Discussion
This study provides a general picture of non-fatal fall victims who sought treatment in emergency care centers. The results suggest that prevention programs and future studies should be priorities in healthcare services. Although the results provide a considerable range of information about victims, circumstances, and places of occurrence, we discuss the issues that we consider the most relevant or most novel.
The majority of the studied fall victims were males, which is normal in studies of injuries due to external causes. However, the male/female ratio depends on the external cause; for example, the ratio is much higher for males in homicides.5 Although falls that require emergency care demonstrate a more even ratio between men and women, the proportional difference between gender is apparent in the mortality and morbidity data for external causes in the public health system.5 The association between falls among individuals over 60 and some type of reported disability (physical or mental) is consistent with the data from the literature, which reports that impaired functional capacity, cognitive disorders, changes in gait, impaired vision, and other disabilities are risk factors for falls in this age group.3,13
The findings from the descriptive study and the correspondence analysis were complementary, especially given that children, adolescents, and youth aged up to 19 represent more than half (56.8%) of all visits. Furthermore, home residences were the most frequent location for falls, which is consistent with the national4,8 and international literature.12 Additionally, the correspondence analysis showed an association between children younger than 9 and falls from beds or other pieces of furniture. Naturally, children spend more of their time at home than the adult population does, so the home is a frequent location for accidents and falls. These results are consistent with children's expected stage of development because they are at a high risk of falling from beds, chairs, sofas, and other furniture. However, studies have shown that simple interventions in the home can be effective in preventing these falls.12,19 In this context, it is important to educate families about supervising their children, especially given that an increasing number of women are in the work force. Healthcare professionals should also be involved in these programs because they play an important role in promoting childcare and children's health.
The association between falls in schools and adolescents in the 10 to 14 age group suggests that homes and schools should be the primary targets for strategies to reduce these occurrences among high-risk groups. For victims between 15 and 19, falls were associated with sports, which is consistent with the data from other countries.6 Young people's participation in sports and other physical activities should be encouraged as part of a healthy life style, and actions that target the schools, clubs, and other venues where such activities take place may help to reduce injuries from falls.
The high frequency of work-related falls, approximately 15% of the total, is worrisome. For victims in the economically active age group (15 to 59 years), this proportion reaches almost 30%. The correspondence analysis showed that most falls from scaffolding and roofs, which affect young adults and adults, occurred at the workplace. These falls caused the most serious health problems, including multiple traumas, head injuries, and injuries to multiple organs. Information about the severity of these accidents represents a knowledge gap in this area. Information from the Ministry of Social Welfare shows that a considerable proportion (80.4%) of the 545,268 Reports of Workers' Compensation filed in 2008 (Comunicações de Acidentes de Trabalho, CAT) were classified as typical, which means that they occurred in the workplace.
Alcohol consumption is widely recognized as a risk factor for injuries due to external causes,2 but little is known about its role in falls. Our results showed that 6.4% of the victims reported having consumed alcohol prior to their fall. This proportion increases to 11.4% when we include the cases where the interviewers suspected alcohol consumption. A study conducted in a hospital in Minas Gerais (southeastern Brazil) showed that a third of trauma patients, mostly males, had consumed alcoholic beverages.2 Proportionally, alcohol use was more frequent in patients who were victims of violence, and this number reached 19.3% for fall victims. The authors also found that most victims of injuries due to external causes after alcohol consumption were not occasional drinkers, but probably chronic users or alcoholics.2
Our study has some limitations and some strengths. One of the limitations is that the data are from a convenience sample and therefore cannot be generalized to Brazil or used to construct rates. Among the strengths, we emphasize our reliable and comprehensive data. A low proportion of our variables showed "no information", ranging from 0.3% for the age group variable and 4.0% for schooling.
The results of this study provide a general picture of the urgent care and emergency service visits that result from falls and identify associations that could not be observed in a descriptive study. It is important to clarify these associations to better understand falls and their contributing factors. Having a broad perspective on urgent care and its characteristics will also increase our understanding of work-related accidents. The information regarding falls from SIM, SIH/SUS and Social Security are underestimated because they are limited to works in formal sector. Therefore, we believe our findings can help to guide fall prevention efforts, particularly strategies to reduce risk factors in homes, schools, and workplaces.
REFERENCES
-
1Centers for Disease Control and Prevention. Self-reported falls and fall-related injuries among persons aged >65 years: United States, 2006. MMWR Morb Mortal Wkly Rep 2008;57(9):225-9.
- 2. Freitas EAM, Mendes ID, Oliveira LCM. Ingestão alcoólica em vítimas de causas externas atendidas em um hospital geral universitário. Rev Saude Publica. 2008;42(5):813-21. DOI:10.1590/S0034-89102008000500005
- 3. Gama ZAS, Gómez-Conesa A. Factores de riesgo de caídas en ancianos: revisión sistemática. Rev Saude Publica 2008;42(5):946-56. DOI:10.1590/S0034-89102008000500022
- 4. Gawryszewski VP, Scarpellini S, Dib JA, Mello Jorge MHP, Pereira Junior GA, Morita M. Atendimentos de emergência por lesões decorrentes de causas externas: características das vítimas e local de ocorrência, Estado de São Paulo, Brasil, 2005. Cad Saude Publica. 2008;24(5):1121-9. DOI:10.1590/S0102-311X2008000500019
- 5. Gawryszewski VP, Monteiro RA, Bandeira de Sá NN, Mascarenhas MDM, Silva MMA;Bernal R, et al. Acidentes e violências no Brasil: um panorama atual das mortes, internações hospitalares e atendimentos em serviços de urgência. In: Ministério da Saúde (BR), Secretaria de Vigilância em Saúde. Saúde Brasil 2009. Brasília (DF); 2010. p.137-173.
- 6. Gilchrist J, Saluja G, Marshall SW. Interventions to prevent sports and recreation-related injuries. In: Doll LS, Bonzo SE, Sleet D, Mercy JA, Haas EN, editors. Handbook of injury and violence prevention. New York: Springer; 2007. p.117-35.
- 7. Kish L. Survey sampling. New York: John Wiley & Sons; 1965. (Wiley Classics Library).
- 8. Malta DC, Mascarenhas MDM, Silva MMA, Macário EM. Perfil dos atendimentos de emergência por acidentes envolvendo crianças menores de dez anos: Brasil, 2006 a 2007. Cienc Saude Coletiva 2009;14(5):1669-79. DOI:10.1590/S1413-81232009000500008
- 9. Mascarenhas MDM, Silva MMA, Malta DC, Moura L, Macário EM, Gawryszewski VP, et al. Perfil epidemiológico dos atendimentos de emergência por violência no Sistema de Serviços Sentinelas de Vigilância de Violências e Acidentes (Viva) - Brasil, 2006. Epidemiol Serv Saúde. 2009;18(1):17-28. DOI:10.5123/S1679-49742009000100003
- 10. Mascarenhas MDM, Silva MMA, Malta DC, Moura L, Gawryszewski VP, Costa VC, et al. Atendimentos de emergência por acidentes na Rede de Vigilância de Violências e Acidentes: Brasil, 2006. Cien Saude Coletiva 2009;14(5):1657-68. DOI:10.1590/S1413-81232009000500007
- 11. Mingoti SA. Análise de dados através de métodos estatísticos multivariados: uma abordagem aplicada. Belo Horizonte: UFMG; 2005.
- 12. Nagaraja J, Menkedick J, Phelan KJ, Ashley P, Zhang X, Lanphear BP. Deaths from residential injuries in US children and adolescents, 1985-1997. Pediatrics 2005;116(2):454-61. DOI:10.1542/peds.2004-1415
- 13. Perracini MR, Ramos LR. Fatores associados a quedas em uma coorte de idosos residentes na comunidade. Rev Saude Publica 2002;36(6):709-16. DOI:10.1590/S0034-89102002000700008
- 14. Ramos EMLS, Almeida SS, Araújo AR, organizadores. Segurança pública: uma abordagem estatística e computacional. Belém: EDUFPA; 2008.
- 15. Santana VS, Xavier C, Moura MCP, Oliveira R, Espírito-Santo JS, Araújo G. Gravidade dos acidentes de trabalho atendidos em serviços de emergência. Rev Saude Publica. 2009;43(5):750-60. DOI:10.1590/S0034-89102009005000061
- 16. Silva NN. Amostragem probabilística: um curso introdutório. 2 ed. São Paulo: EDUSP; 2001.
- 17. Souza AC, Bastos RR, Vieira MT. Análise de correspondência simples e múltipla para dados amostrais complexos. 2010 [citado 2010 ago 18]. Disponível em: http://www.ime.unicamp.br/sinape/sites/default/files/Artigo%20Sinape%20v2.pdf
- 18. STATACORP. Stata survey data reference manual. College Station; 2003.
- 19. Staunton CE, Frumpkin H, Dannenberg AL. Changing the built environment to prevent injury. In: Doll LS, Bonzo SE, Sleet D, Mercy JA, Haas EN, editors. Handbook of injury and violence prevention. New York: Springer; 2007. p.257-275.
The characteristics and factors of emergency service visits for falls
Publication Dates
-
Publication in this collection
27 Mar 2012 -
Date of issue
Feb 2012
History
-
Received
28 Mar 2011 -
Accepted
23 Aug 2011