Abstracts
Although there are not many reports in literature, iliopectineal bursitis presents clinically with signs and symptoms frequently found in outpatient services and practice. Its clinical presentation is anterior hip pain that worsens with the extension, abduction and internal rotation of the hip. The diagnosis is confirmed by ultrasound or magnetic nuclear resonance imaging of the hip. The iliopectineal bursitis responds well to conservative treatment with non-hormonal anti-inflammatory drugs and rest. Due to its good evolution, it is not rare to treat iliopectineal bursitis successfully without even knowing what is being treated.
bursa; iliopectineal bursitis; magnetic resonance imaging
A bursite iliopectínea, embora não tenha muitos relatos na literatura, apresenta-se clinicamente com sinais e sintomas frequentemente encontrados nos ambulatórios e consultórios. Sua clínica é de dor na parte anterior do quadril que piora à extensão, abdução e rotação interna do mesmo. O diagnóstico é confirmado pelo ultrassom ou ressonância nuclear magnética do quadril. A bursite iliopectínea responde bem ao tratamento conservador com anti-inflamatório não hormonal e repouso. Devido a esta boa evolução, não raro, pode-se tratar uma bursite iliopectínea com sucesso sem se saber o que está tratando.
bursa; bursite iliopectínea; ressonância magnética
CASE REPORT
ICoordinator of the Department of Orthopedics and Traumatology of Hospital Unimed Betim. Chief Resident at the Department of Orthopedics and Traumatology and Orthopedist at Hospital Geral Governador Israel Pinheiro - IPSEMG, BH/MG
IIFull Member of Sociedade Brasileira de Ortopedia e Traumatologia. Physician - IPSEMG and Hospital da Polícia Militar de MG
Correspondence to
ABSTRACT
Although there are not many reports in literature, iliopectineal bursitis presents clinically with signs and symptoms frequently found in outpatient services and practice. Its clinical presentation is anterior hip pain that worsens with the extension, abduction and internal rotation of the hip. The diagnosis is confirmed by ultrasound or magnetic nuclear resonance imaging of the hip. The iliopectineal bursitis responds well to conservative treatment with non-hormonal anti-inflammatory drugs and rest. Due to its good evolution, it is not rare to treat iliopectineal bursitis successfully without even knowing what is being treated.
Keywords: bursa, iliopectineal bursitis, magnetic resonance imaging.
INTRODUCTION
The iliopectineal bursa is the largest one in the body. It is located over the iliopectineal eminence anteriorly on the hip,1 between the iliofemoral ligament and the iliopsoas tendon; it extends from the trochanter minor to the iliac fossa, underneath the iliac muscle and is present, bilaterally, in 98% of the adult population.2,3,4 The passage of the iliopsoas tendon over the iliopectineal eminence in the pubis can result in an audible sensation in cases of inflammation.5 Approximately 10% of the patients present a defect in the anterior part of the articular capsule of the hip, allowing the communication of the articular cavity with the bursa.2
The iliopectineal bursitis is frequently associated with hip diseases, such as osteoarthritis, rheumatoid arthritis and sports-related injuries, especially when the pre-exercise warm-up is not performed adequately.6 It can also be secondary to pigmented villonodular synovitis, osteochondromatosis and pyogenic bursitis.2
The signs and symptoms of iliopectineal bursitis are: pain in the anterior part of the hip that worsens with the extension, abduction and internal rotation of the latter. Sometimes it can generate pain in the iliac fossa and, if the pain is located on the right, it can simulate appendicitis. It can also cause irradiated pain along the path of the femoral nerve, by compressing the latter with its distension.2,1,7 The diagnosis is confirmed by ultrasound (US) or nuclear magnetic resonance (NMR) of the hip. US, computed tomography (CT) and NMR show the distended and inflamed bursa, containing hypoechoic fluid at the US, which is hypodense at the CT and has signal intensity similar to that of fluids in all resonance sequences.5 The iliopectineal bursitis responds well to the conservative treatment with non-steroidal anti-inflammatory drugs (NSAIDs) and rest. Corticoid infiltration or local sclerosing agents also constitute part of the therapeutic arsenal and, in selected cases, radiotherapy and even surgery can be used.8,1,7
Saudek9 states that this type of bursitis is associated with hip osteoarthritis, as well as tension of the iliopsoas. The main causes are: trauma, infections, exertion injuries, excessive use of joints, repetitive movements, arthritis (joint inflammation), gout (deposition of uric acid crystals in the joints).
Bonica10 reports moderate to intense pain on the lateral portion of Scarpa triangle and that the femoral nerve, which is affected by the inflammatory process, generates pain in the anterior portion of the thigh and the medial portion of the leg, aggravated when there is tension in the iliopsoas muscle and hip compression.
Signs of pain and edema can be observed at palpation during the examination, which can extend to the inguinal fold.
CASE REPORT
A 45-year-old female patient was seen at the clinic on August 23, 2007, with a complaint of pain in the anterior hip region for two weeks; she did not present initial trauma, fever or concomitant diseases. At physical examination, she presented pain at palpation of the left inguinal region that worsened with extension of the hip. She did not present local flogistic signs or systemic signs of infection.
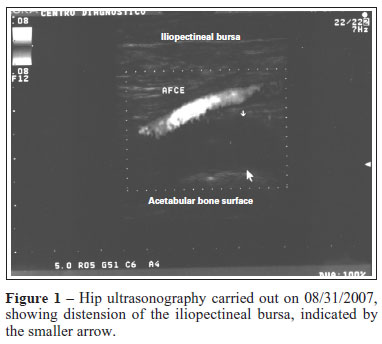
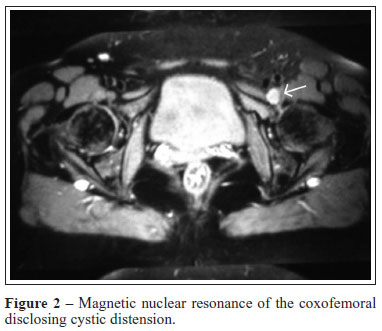
The anteroposterior and frog leg views on the X-ray of the coxofemoral joints showed a slight decrease in the upper joint space bilaterally with subchondral sclerosis. The CT of the coxofemoral joint showed no significant alterations. The hip US (Figure 1) disclosed iliopectineal bursitis to the left, with finding in the topography of the left iliopectineal bursa, rounded anechoic image of thin walls, inferior to the common femoral vessels, corresponding with the painful area reported by the patient. The coxofemoral NMR (Figure 2) showed a cystic distension in the topography of the left iliopectineal bursa, which could be caused by the chronic inflammatory process found in the latter.
The patient was treated with NSAIDs for seven days plus rest and presented clinical improvement of the pain and physical examination with no alterations.
The control US, carried out by the same radiologist, showed a decrease in the cystic image in the iliopectineal topography, observed at the previous echography. The control NMR also showed a decrease in the fluid volume within the iliopectineal bursa.
DISCUSSION
Iliopectineal bursitis is rare in literature reports and no reports have been found in the national literature. However, its signs and symptoms are often found in outpatient clinics and medical offices. The clinical picture consists of anterior hip pain that worsens with the extension, abduction and internal rotation of the hip.
Approximately 10% to 15% of the population presents communication between the iliopectineal bursa and the hip joint.2,7 This condition is often associated with hip pathologies, with a frequency of 30%-40%.1 It can be associated with coxofemoral arthrosis, rheumatoid arthritis, labral injuries, overuse injuries, osteochondromatosis, synovial chondromatosis, pigmented villonodular synovitis, infected bursitis, gout and avascular necrosis of the femur head.1,2
In outpatient clinics, the cases can go unnoticed by a less aware orthopedist, general surgeon, vascular surgeon, gynecologist and general practitioner. Thus, the differential diagnosis includes inflammatory and neoplastic adenopathies, neuromyofascial syndrome, iliopsoas tendinitis, lumbosacral injuries, osteitis pubis, vascular lesions such as aneurysm, pseudoaneurysm of the femoral artery, arteriovenous femoral fistula, hematoma, varicose femoral veins, psoas muscle abscess, neoplasias, femoral or inguinal hernia, cryptorchidism, anterior coxofemoral luxation, appendicitis, etc.1,4
The complementary assessments contribute to the diagnosis the disease. The X-rays can show signs of an underlying pathology, with findings such as subchondral cysts and decreased joint space. Echographically, a cystic mass can be observed in contact with the joint capsule, lateral to the femoral vessels. It can coexist with joint effusion and the use of Doppler can rule out the presence of an aneurysm. The computed tomography can disclose a mass with thin walls and density similar to water, which helps to rule out neoplasias and aneurysms. The NMR, in addition to the diagnosis, can disclose a communication between the bursa and the articular cavity, without the need to perform an arthrography, in addition to a thorough local musculoskeletal assessment.1,2,4
In most of the cases the treatment is conservative, with anti-inflammatory drugs and rest. When this treatment is unsuccessful, or if the clinical signs are intense, a decompressive aspiration of the bursa and injection of steroids or sclerosing agents can be performed. Low-dose radiotherapy has also been reported as treatment for iliopectineal bursitis. The surgical treatment is restricted to conservative treatment failure or recurrence of symptoms and, in these cases, it is the definitive treatment.3,1
In the case reported, as predicted in most cases in the literature, disease regression was observed after the conservative treatment that included rest and anti-inflammatory agents. Thus, it is not rare for iliopectineal bursitis to be treated successfully, whereas being unaware of the nature of the problem.
Beals11 recommends that this syndrome be differentiated from the deep and non-painful click that occurs during the normal mobilization of the hip and does not have clinical significance.
REFERENCES
-
1Urbón MG. Palencia; caso 1. Radiología 1996; 38: 345-71.
-
2Cadera AM. Bursitis iliopsoas (iliopectínea). Disponível em http://www.cto.am.com/bursitis.htm [Acesso em janeiro 2008]
-
3Spalteholz W. Atlas de anatomia humana. Tradução para o espanhol de Dr. E. Pons Tortella. Buenos Aires: Labor, 1944.
-
4Home Therapy. Illiopsoas bursitis and tendonitis anatomy. Disponível em: http://www.aidmybursa.com/illiopsoas-bursitis-anatomy.php [Acesso em dezembro 2007]
-
5Domingues Romeu C, Domingues Rômulo C, Brandão LA. Imagenologia do quadril. Radiol Bras 2001; 34:347-67.
-
6Teixeira MJ, Yeng LT, Fernandes TD, Hernandez AJ, Romano MA, Forni JEN et al. Dor nos membros inferiores. Rev Med 2001; 80(esp. pt.2):391-414.
-
7Tronzo RG. Cirurgía de la cadera. Buenos Aires: Panamericana, 1980.
-
8Turek S. Ortopedia; princípios y aplicaciones. Tomo II. 3.ed. Barcelona: Salvat, 1982.
-
9Saudek CE. O quadril. In: Gould JA. Fisioterapia na ortopedia e na medicina do esporte. 2a.ed. São Paulo: Manole, 1993; p.345-90.
-
10Bonica JJ. The management of pain. Philadelphia: Lea & Febiger, 1990.
-
11Beals RK. Painful snapping hip in young adults. West J Med 1993; 159:481-2.
Iliopectineal bursitis: case report
Publication Dates
-
Publication in this collection
12 Nov 2010 -
Date of issue
Oct 2010
History
-
Received
05 Feb 2009 -
Accepted
15 July 2010