Abstracts
BACKGROUND AND OBJECTIVES: The processed analysis of electroencephalogram became extremely important to monitor nervous system, being used to obtain a better anesthetic adequacy. The objective was to conduct a review about each processed parameter, defining its real importance. CONTENT: A review was conducted showing mathematical, physical and clinical aspects as well as their correlations and updates, presenting new integrated parameters. CONCLUSIONS: An adequate analysis of processed parameters of electroencephalogram may provide more intraoperative safety as well as result in a better outcome for the patient
Consciousness Monitors; Electroencephalography; Electromyography
JUSTIFICATIVA E OBJETIVOS: A análise processada do eletroencefalograma tornou-se de extrema importância na monitoração do sistema nervoso, sendo utilizada a fim de uma melhor adequação anestésica. O objetivo foi fazer uma revisão sobre cada um dos parâmetros processados, definindo sua real importância. CONTEÚDO: Foi realizada revisão mostrando os aspectos matemáticos, físicos e clínicos assim como suas correlações e atualizações, com apresentação de novos parâmetros integrados. CONCLUSÕES: A análise adequada dos parâmetros processados do eletroencefalograma pode proporcionar maior segurança intraoperatória assim como resultar em melhor desfecho para o paciente
MONITORAÇÃO; TÉCNICAS DE MEDIÇÃO; Eletromiografia
JUSTIFICATIVA Y OBJETIVOS: El análisis procesado del electroencefalograma se convirtió en algo extremadamente importante en el monitoreo del sistema nervioso, siendo utilizado para lograr una mejor adecuación anestésica. El objetivo fue realizar una revisión sobre cada uno de los parámetros procesados, definiendo su real importancia. CONTENIDO: Se realizó una revisión mostrando los aspectos matemáticos, físicos y clínicos, como también sus correlaciones y actualizaciones, y presentando nuevos parámetros integrados. CONCLUSIONES: El análisis adecuado de los parámetros procesados del electroencefalograma, puede proporcionar una mayor seguridad intraoperatoria como también un mejor resultado para el paciente
MONITORACIÓN; TÉCNICAS DE MEDICIÓN; Electromiografía
REVIEW ARTICLES
Bispectral index and other processed parameters of electroencephalogram: an update
Rogean Rodrigues NunesI; Itagyba Martins Miranda ChavesII; Júlio César Garcia de AlencarIII; Suyane Benevides FrancoIII; Yohana Gurgel Barbosa Reis de Oliveira III; David Guabiraba Abitbol de MenezesIV
IPhD in Medicine; Graduated in Clinical Engineering; Vice-Coordinator of Ethics Committee in Research of the Hospital São Carlos, Fortaleza, Ceará
IIAnesthesiology Professor of the College of Medicine, Universidade Federal de Juiz de Fora (UFJF-MG)
IIIUndergraduate Medical Student
IVElectrical Engineer, UFC; Graduated in Clinical Engineering
Correspondence to
SUMMARY
BACKGROUND AND OBJECTIVES: The processed analysis of electroencephalogram became extremely important to monitor nervous system, being used to obtain a better anesthetic adequacy. The objective was to conduct a review about each processed parameter, defining its real importance.
CONTENT: A review was conducted showing mathematical, physical and clinical aspects as well as their correlations and updates, presenting new integrated parameters.
CONCLUSIONS: An adequate analysis of processed parameters of electroencephalogram may provide more intraoperative safety as well as result in a better outcome for the patient.
Keywords: Consciousness Monitors; Electroencephalography; Electromyography.
INTRODUCTION
The Greek word for anesthesia (anaisthesia), originally created by Dioscorides in the 1st century of the Christian Era was used by Holmes for the new science emerging in the beginning of 19th century, meaning unconsciousness and sensitivity loss. Anesthesia depth is an old concept 1,2, based on the depressing effects on autonomic nervous system in answer to progressively higher concentrations of anesthetic ether. With incremental doses of inhalational anaesthetic there is a loss of consciousness followed by suppression of autonomic and motor responses to surgical stimuli (nociceptive).
Electroencephalogram (EEG) has been suggested to study intensity of central depression of anesthetics, and its processing has been researched to facilitate its interpretation 3. For this purpose extensive database of EEG readings, coming from patients undergoing different anesthetic regimens, was formed through years.
Electroencephalographic measures of sedation intensity were developed based on observation that in general EEG of an anesthetized patient changes from high frequency low amplitude (HFLA) during consciousness to a low frequency high amplitude (LFHA) when deeply anesthetized.
In the 90s, bispectral analysis, a type of mathematical processing commonly used in geophysics and oil prospection, was used to process the EEG signal. Bispectral index technology (BIS) was developed from a closed algorithm and suggested to monitor brain activity in answer to different combinations of anesthetics.
HOW IS BIS OBTAINED?
BIS (bispectral index) is an index empirically derived and dependent on 'coherency" measurement among components of quantitative electroencephalogram (EEG)3.
SIGNAL CAPTURE
In process of BIS calculation, the first step is acquisition of EEG signal, which is made through application of four electrodes placed on the skin surface that enable an appropriate electrical conduction with low impedance.
The assembly used is the unilateral referencial with exploratory electrode in FT9 or FT10 position (frontal-temporal region) and reference electrode in the FPz position (frontpolar) 4 (Figure 1). This determines that the obtained EEG lineation is monocanal (left or right, according to position of frontal-temporal electrode). Eletrode in the FT8 position is used in BIS algorithm to increase its calculation in the presence of electromyographic activity, and the FP2 electrode (virtual ground) has the purpose of increasing the rejection of common mode.
DIGITALIZATION
Digitalization is performed after acquisition and amplification of signal. The captured analog signal is presented in regular intervals (frequency expressed in Hz) so that deflections of each wave are defined by a series of positive or negative concrete values dependent of the moment of data collection.
The frequency of collected data is essential for obtaining a safe digitalized signal as, according to Shannon's theorem 3,5, it must be superior to double of maximum frequency of the analyzed signal. Maximum frequencies of EEG signal have been considered for a long time, from 30 to 40 Hz, therefore, 70 Hz of frequency would be more real.
If the frequency of samples is small, there is a risk of erroneously converting, a fast analog wave into a slow digitalized wave (aliasing effect) 3.
RECOGNITION AND FILTRATION OF ARTIFACTS
After digitalization, the signal undergoes a process of artifacts recognition 6. The artifacts produced by signals that exceeded dynamic limit of amplifier, like using of electric scalpel, may be identified in epoch (temporal finite divisions of registration, in which analysis is made: two seconds of duration in BIS case) and then are rejected, since original data can not be reconstituted.
Other artifacts can be eliminated from contaminated signal and resulting filtered signal may be used for further analysis. Those types of artifacts include the ones that have frequencies superior to EEG (for instance, alternating electrical current). Other artifacts with frequency within limit of EEG waves, like ECG and the ones produced by rotating pumps (CEC) are eliminated as they present regularity. Other detectable contaminants are interferences produced by stimulators of peripheral nerves as well as the ones emitted by stimulators of evocated potentials. In awake patients or with superficial sedation ocular movements creat a slow recognizable undulatory activity 6.
In BIS specific case, digitalized EEG is filtered to exclude artifacts of high and low frequencies and divided in epochs of two seconds. Each epoch is correlated with an electrocardiogram (ECG) model and in case pacemaker spicules or ECG signals are shown, the same will be eliminated and lost data will be estimated by interpolation. Eyeball movements are detected and epochs contaminated with this artifact, discarded.
Subsequently, the baseline is analyzed and contaminating voltages are eliminated due to low frequencies (for instance, low-frequency noise of electrodes).
TEMPORAL ANALYSIS AND DERIVATIVE PARAMETERS: BURST SUPPRESSION RATIO AND QUAZI SUPPRESSION INDEX
EEG signal after digitalization and filtration of artifacts can be mathematically treated. However, at this moment alterations in voltage can only be evaluated in time domain. From these parameters (voltage and time), many statistical analysis can be carried out resulting in important variables such as: 50% spectral edge frequency (SEF), 95% SEF and much more (strict statistic calculation). For statistical analysis of these data in time domain it is necessary to know that EEG is a non deterministic signal, in other words, it is not possible to exactly predict its future values. Therefore, EEG is a stochastic signal and some statistical points are not predictable 7 (future values can only be previously predicted due to a probability of distribution of amplitudes observed in the signal). Different parameters derived from descriptive temporal statistical analysis have been used, such as EEG electrical power 8, total power 9, analysis described by Hjorth 10 involving activity, mobility and complexity, frequency of crossing (of isoelectric line of zero voltage) and Demetrescu's aperiodic analysis 11 derived from previous parameter.
In BIS calculation it is not used any parameter derived from strict temporal statistical analysis, therefore, its generation is also based in two ad hoc measurements of EEG waves: burst suppression ratio and QUAZI suppression index.
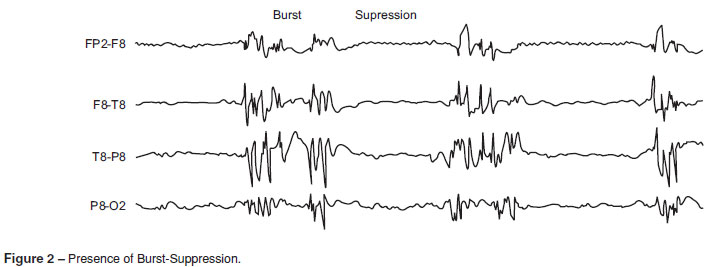
BURST SUPPRESSION RATIO
Suppresion rate is defined as intervals over 0.5 seconds in which EEG voltage is below ± 0.5 µV (Figure 2). Suppression rate 12,13 is the epoch fraction (time period of the analysis of two seconds) in which EEG is isoelectric (does not exceed ± 0.5 µV). Due to the especially variable nature (not stationary) of suppression rate, it must be calculated on average during an interval of at least 30 epochs (60 seconds). Regular suppression ratio is zero.
QUAZI SUPPRESSION RATE
QUAZI suppression rate was projected to discover the presence of suppression rates in the presence of erratic voltage of baseline. QUAZI incorporates information of slow waves (< 1.0 Hz), derived from frequency domain to detect the activity of superimposed rates over these slow waves that would somehow contaminate original algorithm of burst suppression ratio (BSR), exceeding voltage criteria established to define electrical silence. With this index, we can detect certain suppression periods that could not be discovered with strict criteria of electrical silence (± 5 µV) imposed by definition of burst suppression rate.
WINDOW, FREQUENCY ANALYSIS AND DERIVED PARAMETERS: RELATIVE POWER Β
Before carrying out frequency analysis and to avoid errors in subsequent interpretation of waves, due to artificial disruptures in continuous lineation in epochs, each epoch is analyzed according to Blackman window, which reduces distortions related to contamination by frequency artifacts created by abrupt transitions in extremes of each epoch.
After signal digitalization and application of the window function of Blackman 14, the same can be mathematically treated through Fourier analysis. This analysis generates a spectrum of frequencies that corresponds to a simple histogram of amplitudes in the frequency domain.
The best analogy to understand Fourier analysis is to compare EEG with a white light that crosses a crystal prism, creating a rainbow (the spectrum). Each color of light represents a frequency and the luminosity of colors represents the amplitude in each frequency.
In clinical monitors, EEG is decomposed into its frequency spectrum by Fast Fourier Transform (FFT) by Cooley and Tukey 15. This algorithm enables an efficient calculation of digitalized data and is presented graphically as a histogram of power in frequency domain, being discarded the phase spectrum. Quantitative analysis of signal obtained through the FFT enables the identification of some general patterns, called bands, where each is defined by a range of frequencies: δ = 0.5-3.5 Hz, θ = 3.5-7.0 Hz, α = 7.0-13.0 Hz, β = 13.0-30.0 Hz and β2 = 30.0-50.0 Hz.
Different parameters can be derived from the power spectrum: total amplitude or power, relative amplitude or power of bands, frequency of peak power, 50% SEF, 95% SEF and extended delta quotient. There are other parameters that combine temporal with frequency analysis, such as limit spectral frequency compensated with burst suppression [Bc-SEF = (1-BSR/100)] 3.
RELATIVE β POWER
The frequency analysis parameter that uses BIS is the β relative rate, which is defined as log (P30-47 Hz/P11-20 Hz). In other words, it is the logarithm of the quotient between sums of spectral energies (wave amplitude expressed as square voltage) of frequencies bands. Thus, we have a low-frequency band (11-20 Hz), which is included within two classic spectra: α and β and another one of high frequency, included within β2 spectrum.
BISPECTRAL ANALYSIS AND DERIVED PARAMETERS: SYNCHFASTSLOW
Bispectral analysis incorporates information about the phase related to beginning of considered epoch, from different frequencies obtained (Figure 3). Bispectrum measures phase correlation of waves obtained by Fourier analysis among different frequencies. In a simplistic model, the higher the degree of phase coupling, the smaller the number of 'bypass" neurons will be. Bispectral analysis enables to suppress noise Gaussian sources, increasing relationship signal/noise, being able to identify non linear situations important in process of signal generation. Bispectrum is calculated multiplying three complex spectral values (each complex spectral value includes frequency, amplitude and phase information), the spectral value of f1 and f2 primary frequencies by spectral value of modulation frequency (f1+f2). This product is the most important point of bispectral analysis: if in each frequency of tripod (f1, f2 and f1+f2) spectral amplitude is big (there is some sine waive for this frequency) and if phase angles for each of three considered frequencies are aligned, the final product will be big (Figure 4 A). On the contrary, if one of sine components is small or absent, or if phase angles are not aligned, the product will be small (Figure 4 B) 16.

The only group of frequency combinations to calculate bispectrum is a space in wedge (shaded triangle on Figure 4) of frequency facing frequency. The possible combinations out of this triangular wedge are not necessary to the calculation due to symmetry [B(f1,f2) = B(f2,f1)]. In addition to that, a range of possible modulation frequencies (f1+f2) is limited to frequencies < half of sampling frequency.
Bispectrum is expressed in microvolts raised to the third power (µV3) as it is product of three sine waives, each one with an amplitude in microvolts. A value derived from bispectrum is bicoherence, which numerically varies from 0 to 1 proportionally to degree of phase coupling in frequency of considered tripod.
SYNCHFASTSLOW
BIS uses as parameter derived from bispectral analysis fast/ slow synchronization, which is logarithm of quotient between sum of all bispectrum peaks in band from 0.5 to 47 Hz and sum of bispetrum in band from 40 to 47 Hz.
WEIGHTED ANALYSIS OF SUBPARAMETERS
BIS number is obtained from weighted analysis of four sub-parameters: burst suppression ratio, QUAZI suppression, beta relative power and fast/slow synchronization, where it is applied a statistical multivariate model using a non linear function 17,18.
The particular utilization of many subparameters in BIS generation was empirically derived from a database, prospectivelly accumulated, of EEG and sedation scales in which it was used a great variety of anesthetic protocols.
Each of these subparameters presents greater or smaller influence in BIS generation (Figure 5), depending on variations in electrical activity captured by the explorer electrode. So, we have:
1. Fast/slow synchronization - correlates better with answers during moderate sedation or superficial anesthesia. This parameters also correlates well with EEG activation states (excitation phase) and during surgical levels of hypnosis.
2. Relative beta power - this parameter is the most important for calculation algorithm of BIS during superficial sedation.
3. Burst suppression and QUAZI suppression - detect deep anesthesia.
CALCULATION OF BIS ANSWER TIME - DELAY TIME
BIS is internally recalculated in every 0.5 second, using an interval of two seconds with 75% overlap. The value showed on screen is updated every second. BIS used an internal window of change, with duration of 15 seconds (Figure 6). Thus, average time to calculate the BIS answer is half of that, in other words, 7.5 seconds, and can be calculated as follows:
Sum n terms related to an arithmetical progression, we have:
Sn = [(a1 + an) . n] / 2,
Being:
n = number of terms = 16,
a1 = first term = zero,
an = a16 = last term = 15
Emphasizing that terms correspond to seconds elapsed. So, we have:
S16 = [(0 + 15) . 16] / 2 → S16 = 120
However, the analysis must be made by average. Thus, since we have 16 terms, the average will be:
S16/16 = 120/16 → S16/16 = 7.5 seconds
From last BIS versions, it was developed a scale that correlates bispectral index with sedation/hypnosis degree (Table I).
OTHER PROCESSED VARIABLES
1. Electromyography - evaluation of electromyographic activity is made in a frequency range of 70 to 110 Hz.
This electromyographic activity is mathematically transformed in electromyographic power through use of root mean square (RMS). Electromyographic power variable is calculated as sum of all RMS, in the mentioned interval (70-110 Hz), normalized for 0,01 µVRMS and expressed in decibel (dB). For instance:
If RMS (70-110 Hz) = 1 µV;
pEMG = 20 * log (1/0.01) = 40 dB.
The visualization interval, shown in a bar chart is between 30 and 55 dB. It is an important parameter, as it measures electrical activity in facial nerve nucleus (bulbo-pontine region). Normally, during general anesthesia values are located below 30 dB.
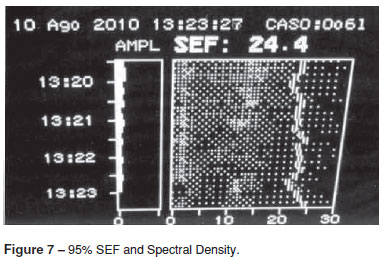
2. Spectral analysis of density (DAS) - corresponds to power density in frequency domain varying from 0 to 30 Hz. The number that represented the limit of spectral edge presents frequency below the point in which 95% of EEG total power is (Figure 7). The analysis of chances in spectral densities shows variations in anesthetic adequacy even if BIS does not vary. Raised percentages of spectral density near the edge (95% SEF) indicate imminent changes in anesthetic adequacy.
3. Mitigation of BIS tendencies - Current versions have three possibilities of mitigation of tendencies, which are obtained through simple mobile averages
19
. This technique consists of calculating arithmetic average of more recent
r
observations (M
t
).
Thus, Mt is an estimate that does not take into account older observations, which is reasonable due to the fact that parameter slightly varies with time. Mobile average name is used because, in each period, the observation is replaced by the most recent one, calculating a new average.
MITIGATION POSSIBILITIES
1. 10 seconds - provides an increased answer to state alterations, such as induction and arousal.
2. 15 seconds - intermediate.
3. 30 seconds - provides a softer tendency, with smaller variability and sensibility to artifacts.
Global view of EEG derivate parameters (Figure 8).
BILATERAL BIS
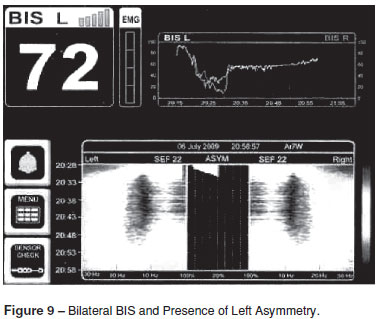
Bilateral BIS shows an important innovation with regard to spectral analysis, since it quantifies automatically another parameter: asymmetry. This one is significative when has relative values over 50% in amplitudes, frequencies or both and has been correlated with neuropathological situations (Figure 9).
CONCLUSION
The correct interpretation of EEG parameters provides more security when making decisions not only related to arousal, whose consequences may result in posttraumatic stress disorder, but also due to the fact that anesthesias with very low BIS values result in negative outcomes 20.
REFERENCES
- 1. Guedel AE - Inalation Anaesthesia: A fundamental Guide, 1st Edition, New York, The Macmillian Company, 1937;1-12.
- 2. Rees GJ, Gray TC - Methyl-N-Propil Ether. Br J Anaesth, 1950;22:83-91.
- 3. Rampill IJ - A primer for EEG signal processing in anesthesia. Anesthesiology, 1998;89:980-1002.
- 4. Johansen JW - Update on bispectral index monitoring. Best Pract Res Clin Anaesthesiol, 2006;20:81-99.
- 5. Shannon CE, Weaver W - The Mathematical Theory of Communication. Urbana, University of Illinois Press, 1962.
- 6. Silva FL, Niedermeyer E - Electroencephalography, 4th Edition, Philadelphia, Lippincott Williams & Wilkins,1999;781-796.
- 7. McEwen J, Anderson GB - Modelling the stationarity and Gaussianity of spontaneous electroencephalographic activity. IEEE Trans Biomed Eng, 1975;22:361-369.
- 8. Bickford RG - Automatic electroencephalographic control of general anesthesia. Electroencephalogr Clin Neurophysiol, 1950;2:93-96.
- 9. Arom KV, Cohen DE, Strobl FT - Effect of intraoperative intervention on neurologic outcome based on electroencephalographic monitoring during cardiopulmonary bypass. Ann Thorac Surg, 1989;48:476-483.
- 10. Hjorth B - EEG analysis based on time domain properties. Electroencephalogr Clin Neurophysiol, 1970;29:306-310.
- 11. Gregory TK, Pettus DC - An electroencephalographic processing algorithm specifically intended for analysis of cerebral electrical activity. J Clin Monit, 1986;2:190-197.
- 12. Rampil IJ, Laster MJ - No correlation between quantitative electroencephalographic measurements and movement response to noxious stimuli during isoflurane anesthesia in rats. Anesthesiology, 1992;77:920-925.
- 13. Rampil IJ, Weiskopf RB, Brown JG et al. - I653 and isoflurane produce similar dose-related changes in the electroencephalogram of pigs. Anesthesiology, 1986;69:298-302.
- 14. Diniz PSR, Da Silva EAB, Netto SL - Processamento Digital de Sinais,1Ş Edição, São Paulo, Bookman, 2002;196-255.
- 15. Cooley JW, Tukey JW - An algorithm for machine calculation of complex Fourier series. Math Computation, 1965;19:297-301.
- 16. Proakis JG, Rader CM, Ling F, Nikias CL - Signal analysis with higher order spectra, Advanced Digital Signal Processing, 1Ş Edition, New York, Macmillan, 1992,550-89.
- 17. Rosow C, Manberg PJ - Bispectral index monitoring. Anesth Clin North Am, 1998;2:89-107.
- 18. Sigl JC, Chamoun NG - An introduction to bispectral analysis for the electroencephalogram. J Clin Monit, 1994;10:392-404.
- 19. Morettin PA, Toloi CMC - Análise de Séries Temporais,1Ş Edição,São Paulo, Edgard Blücher LTDA, 2004;87-108.
- 20. Monk TG, Weldon BC - Anesthetic depth is a predictor of mortality. Anesthesiology, 2010;112:1070-1072.
Publication Dates
-
Publication in this collection
02 Feb 2012 -
Date of issue
Feb 2012
History
-
Received
16 Aug 2010 -
Accepted
19 May 2011