Abstract
The aim of the present study was to search for scientific evidence concerning the association between breastfeeding and bottle feeding and risk of malocclusion in mixed and permanent dentitions. An electronic search was performed in eight databases up to February 2015. Additionally, a gray literature search and hand searches of the reference lists of the selected studies were also carried out. There were no restrictions on language or on year of publication. The methodology of the included articles was evaluated using the Newcastle Ottawa scale. Out of the 817 identified citations, six studies fulfilled the eligibility criteria and were included in the systematic review. One study showed that children with mixed and permanent dentitions breastfed for more than 6 months presented greater mean protrusion of mandibular incisors and inclination of maxillary incisors compared with those breastfed for less than 6 months or those who were bottle-fed (p < 0.05). One study revealed that breastfeeding and bruxism were associated with Class II [OR = 3.14 (1.28 - 7.66)] and Class III [OR = 2.78 (1.21 - 6.36)] malocclusion in children with permanent dentition, while another study showed that an increase in breastfeeding duration was associated with a lower risk of malocclusion in children with both mixed and permanent dentitions (p < 0.001). Three studies did not report any significant association. Risk of bias was high in most selected articles. These findings do not support an association between breastfeeding and bottle feeding and the occurrence of malocclusion in mixed and permanent dentitions.
Malocclusion; Breast Feeding; Bottle Feeding; Dentition, Mixed; Dentition, Permanent
Introduction
Exclusive breastfeeding for at least six months has been highly recommended for preventing gastrointestinal infections and growth deficits in the first months of life.11. Kramer MS, Kakuma R. Optimal duration of exclusive breastfeeding. Cochrane Database Syst Rev. 2012 Aug15;8:CD003517. doi:10.1002/14651858.CD003517.pub2,22. World Heatlh Organization. Exclusive breastfeeding for six months best for babies everywhere. 2011. [cited 2013 Jan 27]. Geneva: HOW; 2011. Available from: http://www.who.int/mediacentre/news/statements/2011/breastfeeding_20110115/en/
http://www.who.int/mediacentre/news/stat...
However, the findings of some studies have confirmed the association between feeding habits and the occurrence of malocclusion in the primary dentition.33. Vázquez-Nava F, Quezada-Castillo JA, Oviedo-Trevino S, Saldivar-González AH, Sánchez-Nuncio HR, Beltrán-Guzmán FJ, et al. Association between allergic rhinitis, bottle feeding, non-nutritive sucking habits, and malocclusion in the primary dentition. Arch Dis Child. 2006;91(10):836-40. doi:10.1136/adc.2005.088484,44. Peres KG, Barros AJ, Peres MA, Victora CG. Effects of breastfeeding and sucking habits on malocclusion in a birth cohort study. Rev Saude Publica. 2007;41(3):343-50. doi:10.1590/l S0034-89102007000300004 Indeed, both breastfeeding and bottle feeding have been associated with a greater chance of cross-bite development when preschool children are evaluated.55. Karjalainen S, Ronning O, Lapinleimu H, Simell O. Association between early weaning, non-nutritive sucking habits and occlusal anomalies in 3-year-old Finnish children. Int J Paediatr Dent. 1999;9(3):169-73. doi:10.1046/j.1365-263x.1999.00133.x,66. Viggiano D, Fasano D, Monaco G, Strohmenger L. Breast feeding, bottle feeding, and non-nutritive sucking; effects on occlusion in deciduous dentition. Arch Dis Child. 2004;89(12):1121-3. doi:10.1136/adc.2003.029728 Moreover, a recent systematic review has shown that the scientific evidence that breastfeeding could protect against malocclusion in the deciduous dentition could not be confirmed.77. Hermont AP, Martins CC, Zina LG, Auad SM, Paiva SM, Pordeus IA. Breastfeeding, bottle feeding practices and malocclusion in the primary dentition: a systematic review of cohort studies. Int J Environ Res Public Health. 2015;12(3):3133-51. doi:10.3390/ijerph120303133
Non-nutritive sucking habits have been suggested to be a cause for malocclusion in mixed88. Montaldo L, Montaldo P, Cuccaro P, Caramico N, Minervini G. Effects of feeding on non-nutritive sucking habits and implications on occlusion in mixed dentition. Int J Paediatr Dent. 2011;21(1):68-73. doi:10.1111/j.1365-263X.2010.01092.x and permanent99. Mistry P, Moles DR, O’Neill J, Noar J. The occlusal effects of digit sucking habits amongst school children in Northamptonshire (UK). J Orthod. 2010;37(2):87-92. doi:10.1179/14653121042939 dentitions. There is also some evidence that bottle feeding,88. Montaldo L, Montaldo P, Cuccaro P, Caramico N, Minervini G. Effects of feeding on non-nutritive sucking habits and implications on occlusion in mixed dentition. Int J Paediatr Dent. 2011;21(1):68-73. doi:10.1111/j.1365-263X.2010.01092.x nail biting, object biting, cheek or lip biting and tooth grinding1010. Thomaz EBAF, Cangussu MCT, Assis AMO. Malocclusion and deleterious oral habits among adolescents in a developing area in northeastern Brazil. Braz Oral Res 2013;27(1):62-9. doi:10.1590/S1806-83242012005000027 during the first years of life may be associated with pacifier use or finger sucking habits in children, which, in turn, can increase the risk of malocclusion. Nevertheless, the association between feeding habits history and malocclusion in mixed and permanent dentitions has been poorly discussed thus far.1111. Narbutyte I, Narbutyte A, Linkeviciene L. Relationship between breastfeeding, bottle-feeding and development of malocclusion. Stomatologija. 2013;15(3):67-72. In addition, there has been no systematic attempt to review and summarize the existing information on this topic.
Therefore, the aim of the present systematic review was to search for scientific evidence of the association between breastfeeding versus bottle feeding and malocclusion in mixed and permanent dentitions. The PICO elements were as follows: children in the mixed and/or permanent dentition stage (patient), bottle feeding (intervention), breastfeeding (comparison), and malocclusion (outcome).
Methodology
Protocol and registration
This systematic review was carried out using the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) checklist as a template.1212. Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group. Preferred reporting items for systematic reviews and meta-analysis: the PRISMA statement. J Clin Epidemiol. 2009;62(10):1006-12. doi:10.1016/j.jclinepi.2009.06.005 Neither a protocol nor a systematic review registration was considered.
Eligibility criteria
The inclusion criteria for this systematic review were epidemiological studies (cross-sectional, case-control, cohort studies and clinical trials) addressing breastfeeding, bottle feeding and mixed feeding (bottle and breastfeeding) and risk of malocclusion in mixed or/and permanent dentitions. Studies on primary dentition conducted with children younger than 7 years; epidemiological studies evaluating outcomes other than malocclusion (dental caries, trauma, temporomandibular disorders); and studies reporting risk factors unrelated to feeding or infancy and the treatment, diagnosis or prevention of malocclusion were excluded. So were literature reviews; letters to the editor; case reports; case series; laboratory studies; studies on food intake; and studies addressing parents’/dentists’ knowledge about oral health.
Information sources
A systematic computerized search was performed up to February 2015 in eight electronic databases: Pubmed (http://www.pubmed.gov), Medline via Ovid (http://gateway.ovid.com), Web of Science (http://www.isiknowledge.com), the Cochrane Library (http://www.cochrane.org/index.htm), Clinical Trials (http://controlled-trial.com), UK National Institute for Health and Care Excellence (http://www.nice.org.uk), US National Institutes of Health (http://www.clinicaltrials.gov) and Lilacs and the Brazilian Library of Dentistry (BBO) through the Virtual Health Library (Bireme, Latin America) (www.bireme.br). There were no restrictions on language or on year of publication. The reference lists of the selected articles were also hand-searched for applicable studies that might have been missed in the computerized searches. Additionally, a partial gray literature search was conducted with OpenGrey and Google Scholar limiting the search to the first 100 most relevant hits. The Reference Manager Software®(Reference Manager, Thomson Reuters, version 12.0.3) was used to organize the list of studies. Duplicate results were removed upon identification.
Search strategy
The following strategy was used in Medline, Pubmed, Web of Science and Cochrane databases: ((malocclusion* OR malocclusion[Mesh] OR dental occlusion[Mesh] OR Maxillofacial Development[Mesh]) AND (bottlefeed* OR bottle feed* OR bottle-feed* OR bottlefed OR bottle fed OR bottle-fed OR “bottle feeding”[Mesh] OR “breast feeding”[Mesh] OR breastfeed* OR breast feed* OR breast-feed* OR breastfed OR breast fed OR breast-fed OR weaning OR “Sucking behavior”[Mesh] OR “Feeding Behavior”[Mesh] OR “risk factors”[Mesh])) NOT (“animals”[Mesh] NOT “humans”[Mesh]). Medline and Pubmed were limited by “humans.” Bireme, Clinical Trials, UK National Institute for Health and Care Excellence and US National Institutes of Health were searched using combined keywords: “bottle feeding”, “breast feeding”, “sucking behavior”, “weaning” and “malocclusion.”
Study selection
The review process was carried out in two phases. In phase 1, two researchers (CCM and LGA) independently reviewed the list of titles and abstracts for inclusion. Once potentially adequate abstracts were selected, full articles were retrieved for a second selection process. If the abstract was judged to contain insufficient information for a decision of inclusion or exclusion, the full text was obtained and reviewed before a final decision was made. In phase 2, the eligibility criteria were applied to the full articles by the same two researchers (CCM and LGA). In both phases, any discrepancies in the inclusion of the articles between researchers were addressed through discussion until consensus was reached.
Data collection process
Two researchers (CCM and LGA) independently extracted data from the articles that met the inclusion criteria and compared their findings for accuracy. They discussed and re-examined any discrepancies until an agreement was reached. When additional or missing information was required, the authors of the articles were contacted.
Data items
Data on the following items were collected: country, study design, initial and final sample, data collection setting, child’s age at the time of the dental examination, how data on feeding habits were collected, how malocclusion was evaluated, statistical analyses, adjustment for confounders, overall result and direction of the effect (statistically significant or not).
The main outcome was malocclusion, which was considered the endpoint of disease (present/absent). Feeding habits were extracted as categorical or numerical variables based on the duration of breastfeeding and bottle feeding, as reported by the authors. Confounders and interactions were extracted and described when evaluated in the multivariate analyses.
Risk of bias in individual studies
The methodological quality was assessed by two researchers (CCM and LGA) using the Newcastle-Ottawa scale for case-control studies and the modified Newcastle-Ottawa scale for cross-sectional ones.1313. Wells GA, Shea B, O’Connell D, Peterson J, Welch V, Losos M, et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomized studies in meta-analyses [Internet]; Ottawa: Ottawa Hospital Research Institute; 2009 [cited 2013 Dec 15]. Available from: www.ohri.ca/programs/clinical_epidemiology/oxford.htm
www.ohri.ca/programs/clinical_epidemiolo...
For the case-control studies, a quality score was calculated based on three major categories: group selection (four items), comparability between groups (one item), and outcome and exposure assessment (three items). A maximum of one point was allocated to each item in the group selection and outcome and exposure assessment categories and a maximum of two points was awarded for comparability. Therefore, the maximum score was nine points and represented the highest methodological quality. For the cross-sectional studies, the score was calculated based on the same three categories. However, those categories had a different number of items: group selection (two items), comparability (one item), and outcome and exposure assessment (two items). Thus, the maximum score was six points and also indicated the highest methodological quality. Any disagreement between researchers was resolved by means of discussion.
Summary measures
Any outcome measure that evaluated the association between breastfeeding and bottle feeding and malocclusion in mixed and permanent dentitions was considered and included odds ratio (OR) and confidence intervals (CI). For the studies in which CI were not provided, p-values were presented.
Synthesis of the results and risk of bias across studies
The heterogeneity among the included studies was evaluated through the examination of various characteristics of the finally selected reports, such as dissimilarity between study participants and outcomes.1414. Higgins JP, Thompson SG. Quantifying heterogneneity in meta-analysis. Stat Med. 2002 Jun;21(11):1539-58. doi:10.1002/sim.1186 If the data were homogeneous and appropriate for pooling, then a meta-analysis would be considered. If the data were heterogeneous and inappropriate for a meta-analysis, a qualitative synthesis would be performed instead.
Additional analysis
Publication bias was considered as an additional analysis.
Results
Study selection
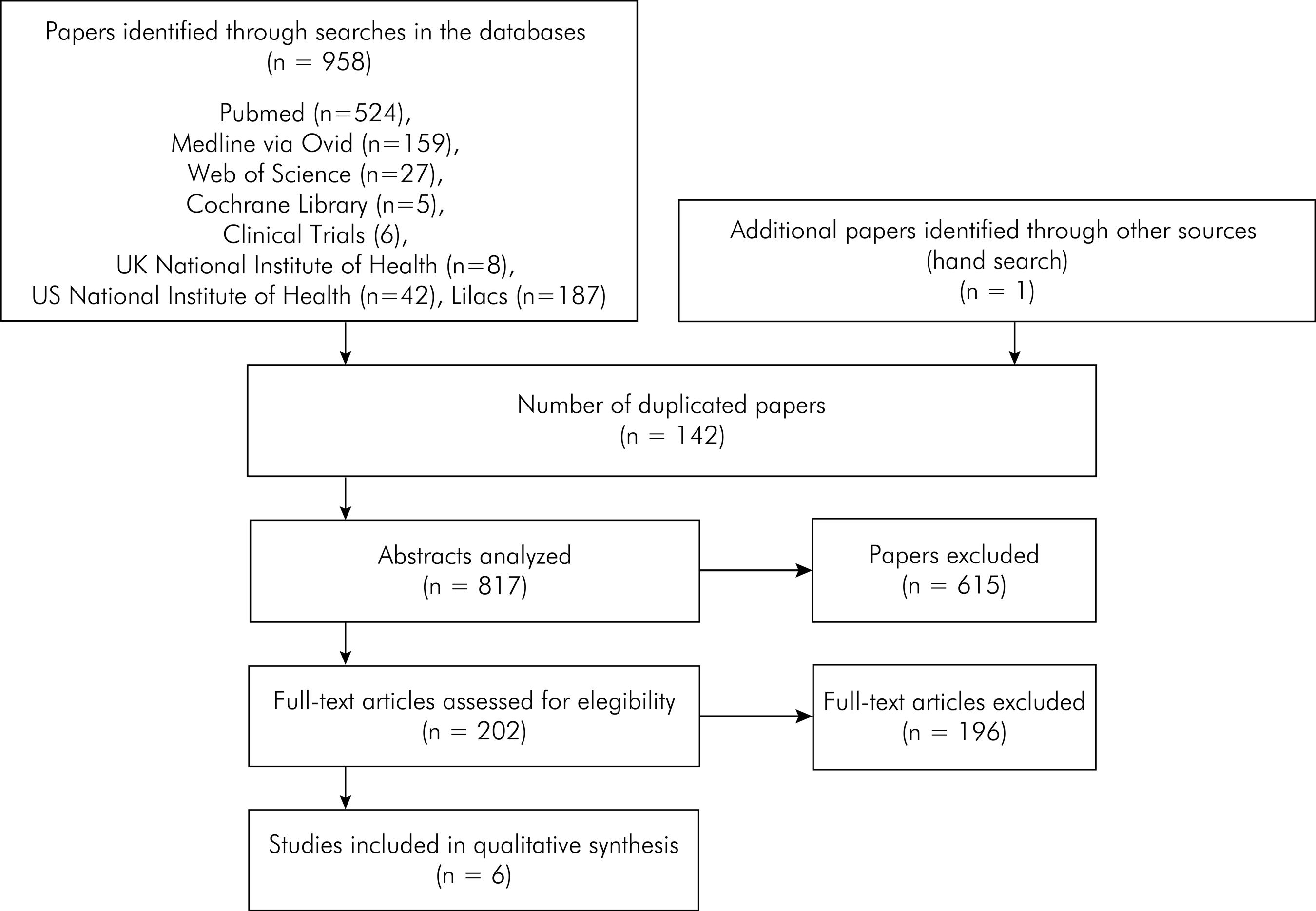
The computerized search yielded 958 references across the eight electronic databases. After removal of duplicate references, 817 titles and abstracts were read and analyzed in phase 1, of which 615 were excluded. Therefore, a total of 202 studies were selected for the analysis of the full texts in phase 2. After reading of the full texts, only six articles1515. Labbok MH, Hendershot GE. Does breast-feeding protect against malocclusion? An analysis of the 1981 Child Health Supplement to the National Health Interview Survey. Am J Prev Med. 1987;3(4):227-32. doi:10.1016/j.earlhumdev.2007.12.008,1616. Meyers A, Hertzberg J. Bottle-feeding and malocclusion: is there an association? Am J Orthod Dentofacial Orthop. 1988;93(2):149-52. doi:10.1016/0889-5406(88)90293-4,1717. Luz CL, Garib DG, Arouca R. Association between breastfeeding duration and mandibular retrusion: a cross-sectional study of children in the mixed dentition. Am J Orthod Dentofacial Orthop. 2006;130(4):531-4. doi:10.1016/j.ajodo.2006.06.011,1818. Nobile CG, Pavia M, Fortunato L, Angelillo IF. Prevalence and factors related to malocclusion and orthodontic treatment need in children and adolescents in Italy. Eur J Public Health. 2007;17(6):637-41.,1919. Sánchez-Molins M, Grau Carbó J, Lischeid Graig C, Ustrell Torrent JM. Comparative study of the craniofacial growth depending on the type of lactation received. Eur J Paediatr Dent. 2010;11(2):87-92.,2020. Thomaz EB, Cangussu MC, Assis AM. Maternal breastfeeding, parafunctional oral habits and malocclusion in adolescents: a multivariate analysis. Int J Pediatr Otorhinolaryngol. 2012;76(4):500-6. doi:10.1016/j.ijporl.2012.01.005 met the eligibility criteria and were included in the present systematic review. A list of the articles excluded in phase 2 along with the reasons for their exclusion is displayed in Appendix 1 and is available upon request. One report was identified through the hand-search of the reference lists. No article was identified through the gray literature search. A flowchart depicting the selection process of the articles at each stage of the systematic review is provided in Figure.
Study characteristics
Among the six articles included in the present systematic review, one was a case-control1616. Meyers A, Hertzberg J. Bottle-feeding and malocclusion: is there an association? Am J Orthod Dentofacial Orthop. 1988;93(2):149-52. doi:10.1016/0889-5406(88)90293-4 study and five were cross-sectional studies.1515. Labbok MH, Hendershot GE. Does breast-feeding protect against malocclusion? An analysis of the 1981 Child Health Supplement to the National Health Interview Survey. Am J Prev Med. 1987;3(4):227-32. doi:10.1016/j.earlhumdev.2007.12.008,1717. Luz CL, Garib DG, Arouca R. Association between breastfeeding duration and mandibular retrusion: a cross-sectional study of children in the mixed dentition. Am J Orthod Dentofacial Orthop. 2006;130(4):531-4. doi:10.1016/j.ajodo.2006.06.011,1818. Nobile CG, Pavia M, Fortunato L, Angelillo IF. Prevalence and factors related to malocclusion and orthodontic treatment need in children and adolescents in Italy. Eur J Public Health. 2007;17(6):637-41.,1919. Sánchez-Molins M, Grau Carbó J, Lischeid Graig C, Ustrell Torrent JM. Comparative study of the craniofacial growth depending on the type of lactation received. Eur J Paediatr Dent. 2010;11(2):87-92.,2020. Thomaz EB, Cangussu MC, Assis AM. Maternal breastfeeding, parafunctional oral habits and malocclusion in adolescents: a multivariate analysis. Int J Pediatr Otorhinolaryngol. 2012;76(4):500-6. doi:10.1016/j.ijporl.2012.01.005 Table 1 provides a summary of their characteristics, including methodological data and relevant findings.
All articles were published in English. One study was a population-based study with data collected from the US National Health Interview Survey (NHIS), representing the American population aged 9 to 17 years.1515. Labbok MH, Hendershot GE. Does breast-feeding protect against malocclusion? An analysis of the 1981 Child Health Supplement to the National Health Interview Survey. Am J Prev Med. 1987;3(4):227-32. doi:10.1016/j.earlhumdev.2007.12.008 One study provided sample size calculation and was representative of a Brazilian city.2020. Thomaz EB, Cangussu MC, Assis AM. Maternal breastfeeding, parafunctional oral habits and malocclusion in adolescents: a multivariate analysis. Int J Pediatr Otorhinolaryngol. 2012;76(4):500-6. doi:10.1016/j.ijporl.2012.01.005 The other four papers involved convenience samples.1616. Meyers A, Hertzberg J. Bottle-feeding and malocclusion: is there an association? Am J Orthod Dentofacial Orthop. 1988;93(2):149-52. doi:10.1016/0889-5406(88)90293-4,1717. Luz CL, Garib DG, Arouca R. Association between breastfeeding duration and mandibular retrusion: a cross-sectional study of children in the mixed dentition. Am J Orthod Dentofacial Orthop. 2006;130(4):531-4. doi:10.1016/j.ajodo.2006.06.011,1818. Nobile CG, Pavia M, Fortunato L, Angelillo IF. Prevalence and factors related to malocclusion and orthodontic treatment need in children and adolescents in Italy. Eur J Public Health. 2007;17(6):637-41.,1919. Sánchez-Molins M, Grau Carbó J, Lischeid Graig C, Ustrell Torrent JM. Comparative study of the craniofacial growth depending on the type of lactation received. Eur J Paediatr Dent. 2010;11(2):87-92. One included participants from a private office,1616. Meyers A, Hertzberg J. Bottle-feeding and malocclusion: is there an association? Am J Orthod Dentofacial Orthop. 1988;93(2):149-52. doi:10.1016/0889-5406(88)90293-4 one included individuals from a university setting,1919. Sánchez-Molins M, Grau Carbó J, Lischeid Graig C, Ustrell Torrent JM. Comparative study of the craniofacial growth depending on the type of lactation received. Eur J Paediatr Dent. 2010;11(2):87-92. one included adolescents from schools of an Italian city,1818. Nobile CG, Pavia M, Fortunato L, Angelillo IF. Prevalence and factors related to malocclusion and orthodontic treatment need in children and adolescents in Italy. Eur J Public Health. 2007;17(6):637-41. and one included individuals from three public schools of a Brazilian city.1717. Luz CL, Garib DG, Arouca R. Association between breastfeeding duration and mandibular retrusion: a cross-sectional study of children in the mixed dentition. Am J Orthod Dentofacial Orthop. 2006;130(4):531-4. doi:10.1016/j.ajodo.2006.06.011
Two studies revealed the existence of malocclusion through parents’ reports,1515. Labbok MH, Hendershot GE. Does breast-feeding protect against malocclusion? An analysis of the 1981 Child Health Supplement to the National Health Interview Survey. Am J Prev Med. 1987;3(4):227-32. doi:10.1016/j.earlhumdev.2007.12.008,1616. Meyers A, Hertzberg J. Bottle-feeding and malocclusion: is there an association? Am J Orthod Dentofacial Orthop. 1988;93(2):149-52. doi:10.1016/0889-5406(88)90293-4 in which parents were asked if a dentist had ever said that their children needed braces or if the parents had perceived that their children needed braces or orthodontic treatment. In three studies, the diagnosis of malocclusion was established in a clinical evaluation performed by calibrated dentists.1717. Luz CL, Garib DG, Arouca R. Association between breastfeeding duration and mandibular retrusion: a cross-sectional study of children in the mixed dentition. Am J Orthod Dentofacial Orthop. 2006;130(4):531-4. doi:10.1016/j.ajodo.2006.06.011,1818. Nobile CG, Pavia M, Fortunato L, Angelillo IF. Prevalence and factors related to malocclusion and orthodontic treatment need in children and adolescents in Italy. Eur J Public Health. 2007;17(6):637-41.,2020. Thomaz EB, Cangussu MC, Assis AM. Maternal breastfeeding, parafunctional oral habits and malocclusion in adolescents: a multivariate analysis. Int J Pediatr Otorhinolaryngol. 2012;76(4):500-6. doi:10.1016/j.ijporl.2012.01.005 In another study, malocclusion was evaluated based on cephalometric data.1919. Sánchez-Molins M, Grau Carbó J, Lischeid Graig C, Ustrell Torrent JM. Comparative study of the craniofacial growth depending on the type of lactation received. Eur J Paediatr Dent. 2010;11(2):87-92. In four studies,1515. Labbok MH, Hendershot GE. Does breast-feeding protect against malocclusion? An analysis of the 1981 Child Health Supplement to the National Health Interview Survey. Am J Prev Med. 1987;3(4):227-32. doi:10.1016/j.earlhumdev.2007.12.008,1616. Meyers A, Hertzberg J. Bottle-feeding and malocclusion: is there an association? Am J Orthod Dentofacial Orthop. 1988;93(2):149-52. doi:10.1016/0889-5406(88)90293-4,1818. Nobile CG, Pavia M, Fortunato L, Angelillo IF. Prevalence and factors related to malocclusion and orthodontic treatment need in children and adolescents in Italy. Eur J Public Health. 2007;17(6):637-41.,2020. Thomaz EB, Cangussu MC, Assis AM. Maternal breastfeeding, parafunctional oral habits and malocclusion in adolescents: a multivariate analysis. Int J Pediatr Otorhinolaryngol. 2012;76(4):500-6. doi:10.1016/j.ijporl.2012.01.005 feeding habits were determined from a questionnaire administered to parents and two studies1717. Luz CL, Garib DG, Arouca R. Association between breastfeeding duration and mandibular retrusion: a cross-sectional study of children in the mixed dentition. Am J Orthod Dentofacial Orthop. 2006;130(4):531-4. doi:10.1016/j.ajodo.2006.06.011,1919. Sánchez-Molins M, Grau Carbó J, Lischeid Graig C, Ustrell Torrent JM. Comparative study of the craniofacial growth depending on the type of lactation received. Eur J Paediatr Dent. 2010;11(2):87-92. failed to report how data on feeding habits were collected.
In general, the studies lacked details, in the Methods section, of approval by the institutional ethics committee.1515. Labbok MH, Hendershot GE. Does breast-feeding protect against malocclusion? An analysis of the 1981 Child Health Supplement to the National Health Interview Survey. Am J Prev Med. 1987;3(4):227-32. doi:10.1016/j.earlhumdev.2007.12.008,1616. Meyers A, Hertzberg J. Bottle-feeding and malocclusion: is there an association? Am J Orthod Dentofacial Orthop. 1988;93(2):149-52. doi:10.1016/0889-5406(88)90293-4,1717. Luz CL, Garib DG, Arouca R. Association between breastfeeding duration and mandibular retrusion: a cross-sectional study of children in the mixed dentition. Am J Orthod Dentofacial Orthop. 2006;130(4):531-4. doi:10.1016/j.ajodo.2006.06.011,1818. Nobile CG, Pavia M, Fortunato L, Angelillo IF. Prevalence and factors related to malocclusion and orthodontic treatment need in children and adolescents in Italy. Eur J Public Health. 2007;17(6):637-41.,1919. Sánchez-Molins M, Grau Carbó J, Lischeid Graig C, Ustrell Torrent JM. Comparative study of the craniofacial growth depending on the type of lactation received. Eur J Paediatr Dent. 2010;11(2):87-92. Nonetheless, all papers had sufficient information for data collection for the systematic review.1515. Labbok MH, Hendershot GE. Does breast-feeding protect against malocclusion? An analysis of the 1981 Child Health Supplement to the National Health Interview Survey. Am J Prev Med. 1987;3(4):227-32. doi:10.1016/j.earlhumdev.2007.12.008,1616. Meyers A, Hertzberg J. Bottle-feeding and malocclusion: is there an association? Am J Orthod Dentofacial Orthop. 1988;93(2):149-52. doi:10.1016/0889-5406(88)90293-4,1717. Luz CL, Garib DG, Arouca R. Association between breastfeeding duration and mandibular retrusion: a cross-sectional study of children in the mixed dentition. Am J Orthod Dentofacial Orthop. 2006;130(4):531-4. doi:10.1016/j.ajodo.2006.06.011,1818. Nobile CG, Pavia M, Fortunato L, Angelillo IF. Prevalence and factors related to malocclusion and orthodontic treatment need in children and adolescents in Italy. Eur J Public Health. 2007;17(6):637-41.,1919. Sánchez-Molins M, Grau Carbó J, Lischeid Graig C, Ustrell Torrent JM. Comparative study of the craniofacial growth depending on the type of lactation received. Eur J Paediatr Dent. 2010;11(2):87-92.,2020. Thomaz EB, Cangussu MC, Assis AM. Maternal breastfeeding, parafunctional oral habits and malocclusion in adolescents: a multivariate analysis. Int J Pediatr Otorhinolaryngol. 2012;76(4):500-6. doi:10.1016/j.ijporl.2012.01.005
Risk of bias in individual studies
The methodological quality evaluation using the Newcastle-Ottawa scale is shown in Tables 2 and 3. The case-control study1616. Meyers A, Hertzberg J. Bottle-feeding and malocclusion: is there an association? Am J Orthod Dentofacial Orthop. 1988;93(2):149-52. doi:10.1016/0889-5406(88)90293-4 scored three points (Table 2). The scores for the cross-sectional studies1515. Labbok MH, Hendershot GE. Does breast-feeding protect against malocclusion? An analysis of the 1981 Child Health Supplement to the National Health Interview Survey. Am J Prev Med. 1987;3(4):227-32. doi:10.1016/j.earlhumdev.2007.12.008,1717. Luz CL, Garib DG, Arouca R. Association between breastfeeding duration and mandibular retrusion: a cross-sectional study of children in the mixed dentition. Am J Orthod Dentofacial Orthop. 2006;130(4):531-4. doi:10.1016/j.ajodo.2006.06.011,1818. Nobile CG, Pavia M, Fortunato L, Angelillo IF. Prevalence and factors related to malocclusion and orthodontic treatment need in children and adolescents in Italy. Eur J Public Health. 2007;17(6):637-41.,1919. Sánchez-Molins M, Grau Carbó J, Lischeid Graig C, Ustrell Torrent JM. Comparative study of the craniofacial growth depending on the type of lactation received. Eur J Paediatr Dent. 2010;11(2):87-92.,2020. Thomaz EB, Cangussu MC, Assis AM. Maternal breastfeeding, parafunctional oral habits and malocclusion in adolescents: a multivariate analysis. Int J Pediatr Otorhinolaryngol. 2012;76(4):500-6. doi:10.1016/j.ijporl.2012.01.005 ranged from one to four points (Table 3).
Results of individual studies
One study showed no significant association between the duration of bottle feeding and the need for orthodontic treatment [OR = 1.73 (CI = 0.82 - 2.10), p = 0.058)].1616. Meyers A, Hertzberg J. Bottle-feeding and malocclusion: is there an association? Am J Orthod Dentofacial Orthop. 1988;93(2):149-52. doi:10.1016/0889-5406(88)90293-4 Another study reported that a longer breastfeeding period was associated with a decreased risk of malocclusion (p < 0.001)1515. Labbok MH, Hendershot GE. Does breast-feeding protect against malocclusion? An analysis of the 1981 Child Health Supplement to the National Health Interview Survey. Am J Prev Med. 1987;3(4):227-32. doi:10.1016/j.earlhumdev.2007.12.008 Only one study adjusted the statistical analysis for confounders and found an interaction between the history of breastfeeding and bruxism, with a synergistic effect on significantly increasing the risk of Angle Class II [OR = 3.14 (CI = 1.28 - 7.66), p < 0.05)] and Class III malocclusion [OR = 2.78 (CI = 1.21 - 6.36), p < 0.05)].2020. Thomaz EB, Cangussu MC, Assis AM. Maternal breastfeeding, parafunctional oral habits and malocclusion in adolescents: a multivariate analysis. Int J Pediatr Otorhinolaryngol. 2012;76(4):500-6. doi:10.1016/j.ijporl.2012.01.005 Based on cephalometric data, children breastfed for more than 6 months had greater mean protrusion of mandibular incisors (p = 0.023) and inclination of maxillary incisors (p = 0.047) in comparison with children who were breastfed for 6 months or less. Children breastfed for more than 6 months also presented a greater mean protrusion of mandibular incisors and inclination of maxillary incisors when compared with bottle-fed children (p < 0.05).1919. Sánchez-Molins M, Grau Carbó J, Lischeid Graig C, Ustrell Torrent JM. Comparative study of the craniofacial growth depending on the type of lactation received. Eur J Paediatr Dent. 2010;11(2):87-92. Two studies did not report any significant association (p > 0.05).1717. Luz CL, Garib DG, Arouca R. Association between breastfeeding duration and mandibular retrusion: a cross-sectional study of children in the mixed dentition. Am J Orthod Dentofacial Orthop. 2006;130(4):531-4. doi:10.1016/j.ajodo.2006.06.011,1818. Nobile CG, Pavia M, Fortunato L, Angelillo IF. Prevalence and factors related to malocclusion and orthodontic treatment need in children and adolescents in Italy. Eur J Public Health. 2007;17(6):637-41.
Synthesis of the results and risk of bias across studies
A meta-analysis was not possible. The six studies included in this systematic review described different types of malocclusion and used different cut-off times to evaluate feeding practices. Therefore, the pooled data from those studies were deemed not suitable because of the differences in the study designs and in the collected information.
Additional analysis
Publication bias was not assessed as there were not enough studies to be entered into a funnel plot.
Discussion
This systematic review attempted to evaluate the association between feeding habits and malocclusion in mixed and permanent dentitions. Oral and craniofacial development may be a health issue on which feeding practices may have a measurable and relevant impact.2121. Davis DW, Bell PA. Infant feeding practices and occlusal outcomes: a longitudinal study. J Can Dent Assoc. 1991;57(7):593-4. Although the first study addressing this topic in schoolchildren and adolescents dates back to more than 25 years, the question remains unanswered and conclusions are yet to be fully confirmed.
One study showed an association between breastfeeding duration and an increased risk of malocclusion,1515. Labbok MH, Hendershot GE. Does breast-feeding protect against malocclusion? An analysis of the 1981 Child Health Supplement to the National Health Interview Survey. Am J Prev Med. 1987;3(4):227-32. doi:10.1016/j.earlhumdev.2007.12.008 while another one did not reveal any statistical significance between feeding habits and malocclusion.1616. Meyers A, Hertzberg J. Bottle-feeding and malocclusion: is there an association? Am J Orthod Dentofacial Orthop. 1988;93(2):149-52. doi:10.1016/0889-5406(88)90293-4 However, those studies lacked a clinical evaluation of malocclusion, which was determined through parents’ reports. The clinical data collected from parents’ reports may be subjective and prone to information bias and, therefore, unreliable.2222. Choi BCK, Pak AWP. A catalog of biases in questionnaires. Prev Chronic Dis [Internet]. 2005 Jan [cited 2008 Mar 13]:2(1)A13. Available from: www.cdc.gov/pcd/issues/2005/jan/04_0050.htm
www.cdc.gov/pcd/issues/2005/jan/04_0050....
One study revealed an interaction between breastfeeding and bruxism, which increased the risk of Class II and Class III malocclusion. This study conducted a multinomial regression analysis, considering gender, age, household income, education level, bottle use, bruxism, digit sucking habit and mouth breathing pattern as confounding variables.2020. Thomaz EB, Cangussu MC, Assis AM. Maternal breastfeeding, parafunctional oral habits and malocclusion in adolescents: a multivariate analysis. Int J Pediatr Otorhinolaryngol. 2012;76(4):500-6. doi:10.1016/j.ijporl.2012.01.005 Adjustment for confounders is very important in epidemiological studies, since an outcome, such as malocclusion, may be associated with multiple risk factors, including gender, genetics, income, feeding practice, non-nutritive sucking habit and other harmful oral habits.2323. McKeever A. Genetics versus environment in the aetiology of malocclusion. Br Dent J. 2012;212(11):527-28. doi:10.1038/sj.bdj.2012.465 Failure to evaluate demographic and clinical factors as potential confounders can bias study results and lead to erroneous conclusions.2424. Skelly AC, Dettori JR, Brodt ED. Assessing bias: the importance of considering confounding. Evid Based Spine Care J. 2012;3(1):9-12. doi:10.1055/s-0031-1298595Also, the methodology of this study was strengthened by the adoption of a representative sample of Brazilian adolescents, allowing the authors to perform a meaningful statistical analysis and to generalize the results for that population.2525. Suresh K, Chandrashekara S. Sample size estimation and Power analysis for clinical research studies. J Hum Reprod Sci. 2012;5(1):7-13. doi:10.4103/0974-1208.97779
When malocclusion was determined based on cephalometric data, greater mean protrusion of the mandibular incisors and inclination of the maxillary incisors seem to occur among children breastfed for more than 6 months in comparison with those breastfed for less than 6 months and those who were bottle-fed.1919. Sánchez-Molins M, Grau Carbó J, Lischeid Graig C, Ustrell Torrent JM. Comparative study of the craniofacial growth depending on the type of lactation received. Eur J Paediatr Dent. 2010;11(2):87-92. Notwithstanding, this study presented the lowest methodology quality and shortcomings with respect to response rate, sample representativeness, control for confounding variables, and selection of individuals with feeding habits.
Some limitations of the present systematic review should be acknowledged. The first one regards the lack of homogeneous data for a meta-analysis. The included studies had different methodologies and different measures for malocclusion, thus hindering the pooling of data.1414. Higgins JP, Thompson SG. Quantifying heterogneneity in meta-analysis. Stat Med. 2002 Jun;21(11):1539-58. doi:10.1002/sim.1186 The second flaw noted during data compilation was the limited number of articles that met our eligibility criteria. Additionally, most evidence found was cross-sectional and no high quality study addressing the association between feeding habits and the occurrence of malocclusion in mixed and permanent dentitions was identified. Finally, the authors of the included articles were unable to group, separately, children who had exclusive breastfeeding or bottle feeding and mixed feeding, making the comparison between those groups impossible. Therefore, breastfeeding and bottle feeding could not be confirmed as risk factors for malocclusion in children and adolescents.
Further research with stronger methodological strategies should be conducted to examine the association between feeding habits and malocclusion in mixed and permanent dentitions. Future studies should also consider the longitudinal design to assess such association more accurately. In cohort evaluations, participants are disease-free at the onset of the study and data regarding exposure to risk factors are collected at distinct points in time before the outcome. Thus, this design enables the assessment of causal hypothesis.2626. Levin KA. Study design IV. Cohort studies. Evid Based Dent. 2006;7(2):51-2. doi:10.1038/sj.ebd.6400407
Conclusion
The findings presented herein do not support an association between breastfeeding and bottle feeding and the occurrence of malocclusion in mixed and permanent dentitions.
The association between feeding practices and this outcome of concern requires additional investigation through prospective cohort studies.
Acknowledgments
This study was supported by the Coordenação de Aperfeiçoamento do Pessoal de Nível Superior - CAPES, Fundação de Amparo à Pesquisa do estado de Minas Gerais - FAPEMIG, Conselho Nacional de Desenvolvimento Científico e Tecnológico - CNPq, and Pró-Reitoria de Pesquisa/Universidade Federal de Minas Gerais - PRPq/UFMG.
References
-
1Kramer MS, Kakuma R. Optimal duration of exclusive breastfeeding. Cochrane Database Syst Rev. 2012 Aug15;8:CD003517. doi:10.1002/14651858.CD003517.pub2
-
2World Heatlh Organization. Exclusive breastfeeding for six months best for babies everywhere. 2011. [cited 2013 Jan 27]. Geneva: HOW; 2011. Available from: http://www.who.int/mediacentre/news/statements/2011/breastfeeding_20110115/en/
» http://www.who.int/mediacentre/news/statements/2011/breastfeeding_20110115/en/ -
3Vázquez-Nava F, Quezada-Castillo JA, Oviedo-Trevino S, Saldivar-González AH, Sánchez-Nuncio HR, Beltrán-Guzmán FJ, et al. Association between allergic rhinitis, bottle feeding, non-nutritive sucking habits, and malocclusion in the primary dentition. Arch Dis Child. 2006;91(10):836-40. doi:10.1136/adc.2005.088484
-
4Peres KG, Barros AJ, Peres MA, Victora CG. Effects of breastfeeding and sucking habits on malocclusion in a birth cohort study. Rev Saude Publica. 2007;41(3):343-50. doi:10.1590/l S0034-89102007000300004
-
5Karjalainen S, Ronning O, Lapinleimu H, Simell O. Association between early weaning, non-nutritive sucking habits and occlusal anomalies in 3-year-old Finnish children. Int J Paediatr Dent. 1999;9(3):169-73. doi:10.1046/j.1365-263x.1999.00133.x
-
6Viggiano D, Fasano D, Monaco G, Strohmenger L. Breast feeding, bottle feeding, and non-nutritive sucking; effects on occlusion in deciduous dentition. Arch Dis Child. 2004;89(12):1121-3. doi:10.1136/adc.2003.029728
-
7Hermont AP, Martins CC, Zina LG, Auad SM, Paiva SM, Pordeus IA. Breastfeeding, bottle feeding practices and malocclusion in the primary dentition: a systematic review of cohort studies. Int J Environ Res Public Health. 2015;12(3):3133-51. doi:10.3390/ijerph120303133
-
8Montaldo L, Montaldo P, Cuccaro P, Caramico N, Minervini G. Effects of feeding on non-nutritive sucking habits and implications on occlusion in mixed dentition. Int J Paediatr Dent. 2011;21(1):68-73. doi:10.1111/j.1365-263X.2010.01092.x
-
9Mistry P, Moles DR, O’Neill J, Noar J. The occlusal effects of digit sucking habits amongst school children in Northamptonshire (UK). J Orthod. 2010;37(2):87-92. doi:10.1179/14653121042939
-
10Thomaz EBAF, Cangussu MCT, Assis AMO. Malocclusion and deleterious oral habits among adolescents in a developing area in northeastern Brazil. Braz Oral Res 2013;27(1):62-9. doi:10.1590/S1806-83242012005000027
-
11Narbutyte I, Narbutyte A, Linkeviciene L. Relationship between breastfeeding, bottle-feeding and development of malocclusion. Stomatologija. 2013;15(3):67-72.
-
12Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group. Preferred reporting items for systematic reviews and meta-analysis: the PRISMA statement. J Clin Epidemiol. 2009;62(10):1006-12. doi:10.1016/j.jclinepi.2009.06.005
-
13Wells GA, Shea B, O’Connell D, Peterson J, Welch V, Losos M, et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomized studies in meta-analyses [Internet]; Ottawa: Ottawa Hospital Research Institute; 2009 [cited 2013 Dec 15]. Available from: www.ohri.ca/programs/clinical_epidemiology/oxford.htm
» www.ohri.ca/programs/clinical_epidemiology/oxford.htm -
14Higgins JP, Thompson SG. Quantifying heterogneneity in meta-analysis. Stat Med. 2002 Jun;21(11):1539-58. doi:10.1002/sim.1186
-
15Labbok MH, Hendershot GE. Does breast-feeding protect against malocclusion? An analysis of the 1981 Child Health Supplement to the National Health Interview Survey. Am J Prev Med. 1987;3(4):227-32. doi:10.1016/j.earlhumdev.2007.12.008
-
16Meyers A, Hertzberg J. Bottle-feeding and malocclusion: is there an association? Am J Orthod Dentofacial Orthop. 1988;93(2):149-52. doi:10.1016/0889-5406(88)90293-4
-
17Luz CL, Garib DG, Arouca R. Association between breastfeeding duration and mandibular retrusion: a cross-sectional study of children in the mixed dentition. Am J Orthod Dentofacial Orthop. 2006;130(4):531-4. doi:10.1016/j.ajodo.2006.06.011
-
18Nobile CG, Pavia M, Fortunato L, Angelillo IF. Prevalence and factors related to malocclusion and orthodontic treatment need in children and adolescents in Italy. Eur J Public Health. 2007;17(6):637-41.
-
19Sánchez-Molins M, Grau Carbó J, Lischeid Graig C, Ustrell Torrent JM. Comparative study of the craniofacial growth depending on the type of lactation received. Eur J Paediatr Dent. 2010;11(2):87-92.
-
20Thomaz EB, Cangussu MC, Assis AM. Maternal breastfeeding, parafunctional oral habits and malocclusion in adolescents: a multivariate analysis. Int J Pediatr Otorhinolaryngol. 2012;76(4):500-6. doi:10.1016/j.ijporl.2012.01.005
-
21Davis DW, Bell PA. Infant feeding practices and occlusal outcomes: a longitudinal study. J Can Dent Assoc. 1991;57(7):593-4.
-
22Choi BCK, Pak AWP. A catalog of biases in questionnaires. Prev Chronic Dis [Internet]. 2005 Jan [cited 2008 Mar 13]:2(1)A13. Available from: www.cdc.gov/pcd/issues/2005/jan/04_0050.htm
» www.cdc.gov/pcd/issues/2005/jan/04_0050.htm -
23McKeever A. Genetics versus environment in the aetiology of malocclusion. Br Dent J. 2012;212(11):527-28. doi:10.1038/sj.bdj.2012.465
-
24Skelly AC, Dettori JR, Brodt ED. Assessing bias: the importance of considering confounding. Evid Based Spine Care J. 2012;3(1):9-12. doi:10.1055/s-0031-1298595
-
25Suresh K, Chandrashekara S. Sample size estimation and Power analysis for clinical research studies. J Hum Reprod Sci. 2012;5(1):7-13. doi:10.4103/0974-1208.97779
-
26Levin KA. Study design IV. Cohort studies. Evid Based Dent. 2006;7(2):51-2. doi:10.1038/sj.ebd.6400407
Publication Dates
-
Publication in this collection
2016
History
-
Received
11 June 2015 -
Reviewed
14 Oct 2015 -
Accepted
24 Nov 2015