Abstract
The study was carried out in a Brazilian population and the aim was to describe the prevalence and the clinic-radiographical features of jaw lesions. In addition, a comparison between the main diagnosis hypothesis and final diagnosis was accessed. A prospective study which evaluated all patients with jaw lesions diagnosed in an Oral Diagnosis Center, between August 2013 and October 2014. A total of 450 patients were observed for the first time, and 130 had some type of jaw lesion. The mean age of the patients was 35.2 years ± 17.86. Among these, 71 were women (54.62%) and 87 were Caucasian (66.92%). The mandible was affected more frequently (71.43%) than the maxilla (28.57%). Swelling and pain were the most frequent clinical signs and symptoms and were observed in 60 (42.85%) and 38 (27.14%) cases, respectively. The panoramic x-ray was the main radiographic exam utilized (88.57%). Radiolucent lesions accounted for 89 cases (63.57%) and the unilocular form was present in 114 cases (81.43%). A total of 93 cases had histopathological analyses and the periapical cyst was the most frequent lesion. In the other 47 lesions, the diagnosis was conducted by clinical and radiographic management. Bone lesions were frequent, being noted on first visit in approximately 30% of patients; in 1/3 of the cases, the diagnoses were completed with a combination of clinical and radiographic exams.
Jaw; Odontogenic Tumors; Odontogenic Cysts; Biopsy; Bone Diseases
Introduction
Studies of jaw lesions (JL) have a fundamental role in dentistry where the dentist is, in most cases, responsible for its diagnosis and treatment. Interestingly, most of these lesions are usually discovered during routine radiographs or when the patient reports a swelling in their jaw and a panoramic x-ray is performed. In general, painful symptoms are not a common finding.11. Neyaz Z, Gadodia A, Gamanagatti S, Mukhopadhyay S. Radiographical approach to jaw lesions. Singapore Med J. 2008;49(2):165-76.
Most of the information regarding JL is from retrospective studies, which evaluated histopathological lab data. The prevalence of odontogenic tumors, mainly ameloblastomas and keratocystic odontogenic tumors (KOT), has been studied in many parts of the world, and differences in prevalence are observed between countries and between center types (Medical and Dental). African studies show a higher prevalence of ameloblastoma than North American studies.22. Arotiba JT, Ogunbiyi JO, Obiechina AE. Odontogenic tumours: a 15-year review from Ibadan, Nigeria. Br J Oral Maxillofac Surg. 1997;35(5):363-7. doi: 10.1016/S0266-4356(97)90411-3
https://doi.org/10.1016/S0266-4356(97)90...
,33. Adebayo ET, Ajike SO, Adekeye EO. A review of odontogenic tumors in Kaduna, Nigeria. J Oral Maxillof Surg. 2005;63(6):811-9. doi:10.1016/j.joms.2004.03.022
https://doi.org/10.1016/j.joms.2004.03.0...
,44. Costa DOP, Maurício AS, Faria PAS, Silva LE, Mosqueda-Taylor A, Lourenço SQC. Odontogenic tumors: A retrospective study of four Brazilian diagnostic pathology center. Med Oral Patol Oral Cir Bucal. 2012;17(3):e389-94. doi:10.4317/medoral.17630
https://doi.org/10.4317/medoral.17630...
Fregnani et al.55. Fregnani ER, Fillipi RZ, Oliveira CR, Vargas PA, Almeida OP. Odontomas and ameloblastomas: variable prevalences around the world? Oral Oncol. 2002;38(8):807-8. doi:10.1016/S1368-8375(02)00050-7
https://doi.org/10.1016/S1368-8375(02)00...
(2002) concluded that ameloblastomas are the main odontogenic tumor treated in medical hospitals, whereas odontomas are observed more frequently in dentistry clinics and dental hospitals. However, for a large number of other jaw lesions, such as osseous dysplasia (OD), bone sclerosis, and simple bone cysts, histopathological exams are not typically performed, and their prevalence is not well established. Consequently, a prospective analysis (determination of prevalence is more reliable) with descriptive epidemiology and clinical and radiographic correlation is essential to determine the actual frequency of JL.
The aim of the present study was to evaluate the clinical and radiographic features of JL diagnosed in a single Institution. In addition, the rate of correct diagnosis was also assessed through comparison of the main diagnosis hypothesis (performed by a stomatologists) with the final diagnosis of each case.
Methodology
This prospective observational study took place at the Oral Diagnosis Center. All of the consecutive patients who had jaw lesions were recruited between August 2013 and October 2014. The Ethics Committee of the Institution approved this research (no. 350.887). All of the patients signed the informed consent and received a copy.
For diagnosis or for biopsy planning, one or multiple radiographic exams were performed according to the lesion indication. Indeed, some data were collected from x-ray (periapical, occlusal and panoramic) or helical computed tomography (CT).
Research criteria
The inclusion criteria included patients with JL observed during the period of the study and came to our clinic for the first time.
The following clinical and radiographic features were collected:
-
clinical: demographic data, signs (mucosal ulceration, bleeding, purulent drainage, and swelling) and symptoms (pain and paresthesia);
-
imaging: site of the lesion, radiodensity/radiolucency/mixed, unilocular/multilocular form, relationship of the lesion with dental apex, root resorption, dental displacement, impacted tooth, displacement of the mandibular canal, and expansion and/or disruption of the cortical bone.
The maxilla and mandible were divided to describe the lesion site:
-
the maxilla was divided into two anatomic regions: anterior (right canine to the left canine) and posterior (first premolar to the maxillary tuberosity);
-
the mandible was divided into five anatomic regions: symphysis (right canine to the left canine), body, angle, ramus, condylar and coronoid processes.
In cases for which biopsy was indicated, the specimens were submitted to the Oral Pathology Lab of the same Institution. The odontogenic cysts and tumors were classified according to the World Health Organization (WHO) criteria.66. Kramer IRH, Pindborg JJ, Shear M. Histological typing of odontogenic tumours. 2nd ed. Berlin: Springer; 1992.,77. Barnes L, Eveson JW, Reichart P, Sidransky D, editors. Pathology and genetics: head and neck tumours. Lyon: IARC Press; 2005. Chapter 6, Odontogenic tumours; p. 283-328. (World Health Organization classification of tumours). To evaluate the rate of correct diagnosis, the main diagnosis hypothesis was compared to the final diagnosis (histopathological exam). The hypothesis was elaborated by a graduate student and a professor (stomatologists) simultaneously. The cases that did not receive a surgical procedure were excluded and divided into 2 subgroups:
-
Group 1: lesions with histopathological confirmation;
-
Group 2: lesions without histopathological evaluation but for which a surgical procedure was performed and no material (tissue) were collected.
Statistical analysis
Descriptive statistics were used to report the results. Qualitative variables were presented in absolute and relative frequencies. The main summary measures of the mean, standard deviation, minimum and maximum values for quantitative variables were presented. The statistical software R version 3.0.1 was used for analyses.
Results
Clinical features
A total of 997 patients were evaluated during the study period (15 months). A total of 450 patients (approximately 45%) were observed for the first time, and 130 (29%) of the latter had a JL.
A total of 140 JL were observed in the 130 patients. Of the patients, 71 were women (54.62%), and 59 were men (45.38%). The patient ages ranged between 8 and 77 years (mean 35.2 ± 17.86), and most patients were Caucasian (66.92%). Regarding the location of the lesions, 3 florid osseous dysplasias and 2 bone scleroses affected both the mandible and the maxilla. Of the other 135 lesions, 95 (67.86%) were located in the mandible and 40 were in the maxilla (28.57%). It is noteworthy that some extensive lesions reached more than one region. In the maxilla, 6 cases involved the anterior and posterior region; in the mandible, 8 lesions involved the symphysis and body, 6 involved the body, angle and ramus, and 1 lesion affected the condylar and coronoid processes. The most frequently signs and symptoms were swelling in 60 cases (42.85%), pain in 38 cases (27.14%), and purulent drainage in 16 cases (11.43%). Other less frequent included bleeding and ulceration of the mucosa adjacent to the bone (Table 1).
Radiographic features
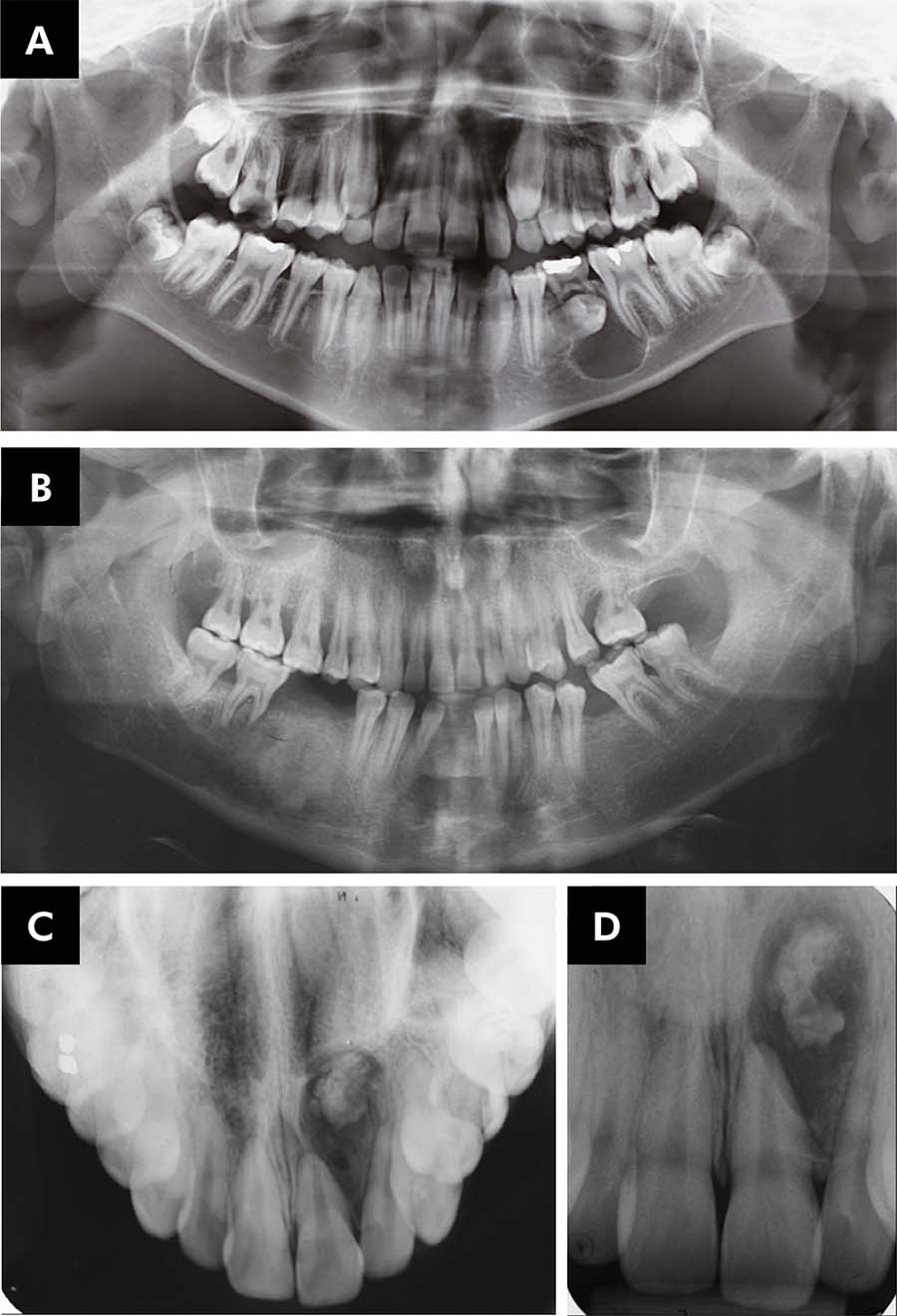
The panoramic x-ray was the exam most frequently used and was performed in 124 cases, followed by periapical x-ray (55 cases), CT (29 cases) and occlusal x-ray (27 cases). Considering the radiographic aspect, 89 out of 140 lesions (63.57%) were exclusively radiolucent, 34 (24.29%) were exclusively radiopaque, and 17 cases (12.14%) were computed as mixed lesions (Figure 1).
(A) Panoramic x-ray showing a radiolucent lesion involving the crown of the tooth 35 (Dentigerous cyst). (B) Poor delimited radiopaque lesion in right mandible (osteosarcoma). (C,D) An occlusal and periapical x-ray showing a mist lesion involving the anterior region of the maxilla (calcifying cystic odontogenic tumor).
A total of 106 lesions (only mixed and radiolucent lesions) were considered for the analysis of the unilocular or multilocular pattern. Of these, 95 were unilocular (84 radiolucent and 11 mixed) and 11 were multilocular (5 radiolucent and 6 mixed). The tooth association showed that 101 lesions (72.14%) had involvement of the dental apex, and 4 of these caused root resorption (1 calcifying cystic odontogenic tumor – CCOT, 1 mucoepidermoid carcinoma – MEC, 1 dentigerous cyst and 1 ameloblastoma), and 23 cases (16.43%) were associated with an impacted tooth (12 dentigerous cysts, 4 odontomas, 4 KOT, 2 CCOT and 1 ameloblastoma). Dental displacement was observed in 20 lesions (10 periapical cysts, 3 odontomas, 2 KOT, 2 ameloblastomas, 2 dentigerous cysts and 1 CCOT).
The following data were evaluated only for the 29 CT: cortical bone expansion was observed in 11 cases (37.93%, 3 periapical cysts, 2 dentigerous cysts, 2 KOT, 1 odontoma, 1 bone exostosis, 1 residual cyst, and 1 ossifying fibroma), cortical disruption in 6 cases (20.69%, 4 periapical cysts, 1 KOT and 1 osteonecrosis) and displacement of the mandibular canal in 3 cases (10.34%, 1 dentigerous cyst, 1 KOT and 1 osteomyelitis).
Surgical data and diagnosis
Surgical procedures were performed for 105 lesions and included 20 incisional biopsies, 73 lesion enucleations and 12 surgical interventions for bleeding stimulation (all cases were simple bone cysts). It is noteworthy that in the latter cases, there was no material available for histopathological analysis. In the other 35 lesions, the diagnosis was performed according to the clinical and imaging features, and biopsy was not indicated. Consequently, there was no histopathological confirmation in the 47 lesions (32.86%). Of these, 16 were osseous dysplasia, 9 were bone sclerosis, and 5 were condensing osteitis; bone exostosis, fibrous dysplasia, multiple myeloma, Stafne bone defect and sinus hypoplasia accounted for 1 case each (Figure 2).
(A-C) Sinus hypoplasia observed in both panoramic x-ray and CT. The CT was crucial for the diagnosis.
Of the 93 cases with histopathological analysis, 38 were periapical cysts, 12 dentigerous cysts, 9 odontomas (7 compounds and 2 complexes), 8 KOT, 6 residual cysts, 5 ameloblastomas and other lesions. There were only 2 cases of malignant tumors, which were osteosarcoma and mucoepidermoid carcinoma (Figure 3).
Odontoma was the most frequent odontogenic tumor observed, and of the 9 represented cases, 7 were compound (4 in the mandible: 2 in the symphysis, and 2 in the body. 3 in the maxilla: 2 in the anterior region and one in the posterior) and 2 were complex (both in the maxilla: 1 in the anterior region and 1 in the posterior region). In regards to the radiographic aspect, 3 were radiopaque, 6 were mixed, and all 9 were unilocular. KOT was the second most frequent odontogenic tumor observed and represented 8 cases; all of them were radiolucent and unilocular. The ameloblastoma was the third, which was observed in 5 cases. All of the cases were radiolucent, with 4 multilocular and 1 unilocular. Periapical cyst was the most frequent odontogenic cyst and represented 38 cases; all cases were radiolucent. Dentigerous cyst was the second most frequent with 12 cases. Malignant tumors represented 3 cases (osteosarcoma, mucoepidermoid carcinoma and multiple myeloma). All of the cases had swelling and cortical disruption, and the case of osteosarcoma presented paresthesia.
Osseous dysplasia was observed in 16 cases, of which 11 (68.75%) were classified as florid. Afro-descendent women were more affected, and the lesions had radiopaque and mixed aspect. Of the 16 lesions, 9 were exclusively radiopaque (5 florid, 3 focal and 1 periapical) and 7 were mixed (6 florid and 1 focal). A simple bone cyst was observed in 12 cases, and all of the cases affected the mandible. Bone sclerosis occurred in 9 cases. As well as simple bone cyst, all of the cases were radiographic findings.
In the Group 1, 79 out of 93 lesions (76.82%) had the main clinical-radiographic diagnosis hypothesis confirmed. In Group 2, a total of 12 lesions had a surgical intervention, but there was no material to be collected. In addition, this characteristic associated to the clinical-radiographic feature was strongly indicative of the diagnosis of SBC. The diagnosis hypothesis was corrected in 11 of the cases (91.67%) (Table 2). The rate of correct diagnosis including Group 1 and 2 was 85.7%.
Discussion
Most JL studies are retrospective, and they usually report data from histopathology labs. However, some entities (osseous dysplasias, bone sclerosis and others) do not require a biopsy to confirm the diagnosis. Consequently, these lesions may be underreported in the literature. In addition, JL represent a wide spectrum of diseases/alterations, and epidemiological studies simultaneously evaluating all of these lesions are uncommon. In general, the data are presented according to the following groups: odontogenic cysts and tumors33. Adebayo ET, Ajike SO, Adekeye EO. A review of odontogenic tumors in Kaduna, Nigeria. J Oral Maxillof Surg. 2005;63(6):811-9. doi:10.1016/j.joms.2004.03.022
https://doi.org/10.1016/j.joms.2004.03.0...
,88. Mosqueda-Taylor A. New findings and controversies in odontogenic tumors. Med Oral Patol Oral Cir Bucal. 2008;13(9):E555-8.,99. Nuñez-Urrutia S, Figueiredo R, Gay-Escoda C. Retrospective clinicopathological study of 418 odontogenic cysts. Med Oral Patol Oral Cir Bucal. 2010;15(5):e767-73. doi:10.4317/medoral.15.e767
https://doi.org/10.4317/medoral.15.e767...
,1010. Avelar RL, Primo BT, Pinheiro-Nogueira CB, Studart-Soares EC, Oliveira RB, Romulo de Medeiros J et al. Worldwide incidence of odontogenic tumors. J Craniofac Surg. 2011;22(6):2118-23. doi:10.1097/SCS.0b013e3182323cc7
https://doi.org/10.1097/SCS.0b013e318232...
, fibro-osseous lesions1111. Macdonald-Jankowski DS. Focal cemento-osseous dysplasia: a systematic review. Dentomaxillofac Radiol. 2008;37(6):350-60. doi:10.1259/dmfr/31641295
https://doi.org/10.1259/dmfr/31641295...
,1212. Worawongvasu R, Songkampol K. Fibro-osseous lesions of the jaws an analysis of 122 cases in Thailand. J Oral Pathol Med. 2010;39(9):703-8. doi:10.1111/j.1600-0714.2010.00932.x
https://doi.org/10.1111/j.1600-0714.2010...
,1313. Santos Netto JN, Cerri JM, Miranda AMM, Pires FR. Benign fibro-osseous lesions: clinicopathologic features from 143 cases diagnosed in an oral diagnosis setting. Oral Surg Oral Med Oral Pathol Oral Radiol. 2013;115(5):e56-65. doi:10.1016/j.oooo.2012.05.022
https://doi.org/10.1016/j.oooo.2012.05.0...
, malignant tumors1414. Perez DEC, Pires FR, Lopes MA, Almeida OP, Kowalski LP. Adenoid cystic carcinoma and mucoepidermoid carcinoma of the maxillary sinus: report of a 44-year experience of 25 cases from a single institution. J Oral Maxillofac Surg. 2006;64(11):1592-7. doi:10.1016/j.joms.2005.11.088
https://doi.org/10.1016/j.joms.2005.11.0...
,1515. Bachar G, Goldstein D, Brown D, Tsang R, Lockwood G, Perez-Ordonez B et al. Solitary extramedullary plasmacytoma of the head and neck: long-term outcome analysis of 68 cases. Head Neck. 2008;3098):1012-9. doi:10.1002/hed.20821
https://doi.org/10.1002/hed.20821...
,1616. Kamal M, Kaur P, Gupta R, Gupta S, Singh S. Mandibular plasmacytoma of jaw: a case report. J Clin Diagn Res. 2014;8(8):ZD20-1. doi:10.7860/JCDR/2014/9565.4674
https://doi.org/10.7860/JCDR/2014/9565.4...
,1717. Stewart BD, Reith JD, Knapik JA, Chi AC. Bone and cartilage-forming tumors and ewing sarcoma: an update with a gnathic emphasis. Head Neck Pathol. 2014;8(4):454-62. doi:10.1007/s12105-014-0587-8
https://doi.org/10.1007/s12105-014-0587-...
, and osteonecrosis1818. Marx RE. Osteoradionecrosis: a new concept of its pathophysiology. J Oral Maxillofac Surg. 1983;41(5):283-8. doi:10.1016/0278-2391(83)90294-X
https://doi.org/10.1016/0278-2391(83)902...
. The present study was prospectively designed with the purpose of determining the prevalence of these types of lesions. Additionally, the main radiographic features were assessed, and the data may be important to elaborate strategies for patient care and teaching in undergraduate programs.
A retrospective study revised data from 40,000 oral biopsies performed in the Canadian population during a period of 26 years. Cysts and odontogenic tumors consisted of 7,324 lesions (18.31%). Interestingly, the authors emphasized that the small number of OD observed represented a bias due to the reluctance to biopsy this condition.1919. Daley TD, Wysocki GP, Pringle GA. Relative incidence of odontogenic tumors and oral and jaw cysts in a Canadian population. Oral Surg Oral Med Oral Pathol. 1994;77(3):276-80. doi:10.1016/0030-4220(94)90299-2
https://doi.org/10.1016/0030-4220(94)902...
In the present study, 450 patients were observed for the first time during the 15 months of the study, and 130 of them (29%) had JL. It is worth noting that there was no histopathological examination in 47 cases (44 patients), which represents approximately a third of all cases. Of these, the diagnosis was performed through clinical and radiographic features in 35 cases, and a surgical procedure was indicated, but there was no material to be collected in the remaining 12 cases. According to the clinical, radiographic, and surgical intervention features, these cases were diagnosed as simple bone cysts. The remaining 93 cases had their diagnosis confirmed by histopathological examination. Cysts (both non-odontogenic and odontogenic) and odontogenic tumors were the main lesions with 58 (41.4%) and 25 cases (17.8%), respectively. Periapical (38 cases – 65.5%) and dentigerous cysts (12 cases – 20.7%) were the most frequent. A retrospective study evaluated 418 cases of odontogenic cysts in the period from 1997 to 2006 and found that 210 cases were periapical cysts (50.2%) and 91 (21.8%) were dentigerous cysts.99. Nuñez-Urrutia S, Figueiredo R, Gay-Escoda C. Retrospective clinicopathological study of 418 odontogenic cysts. Med Oral Patol Oral Cir Bucal. 2010;15(5):e767-73. doi:10.4317/medoral.15.e767
https://doi.org/10.4317/medoral.15.e767...
There are a large number of odontogenic tumors; more than 20 types according to the WHO (2005). Some studies have shown ameloblastoma22. Arotiba JT, Ogunbiyi JO, Obiechina AE. Odontogenic tumours: a 15-year review from Ibadan, Nigeria. Br J Oral Maxillofac Surg. 1997;35(5):363-7. doi: 10.1016/S0266-4356(97)90411-3
https://doi.org/10.1016/S0266-4356(97)90...
,33. Adebayo ET, Ajike SO, Adekeye EO. A review of odontogenic tumors in Kaduna, Nigeria. J Oral Maxillof Surg. 2005;63(6):811-9. doi:10.1016/j.joms.2004.03.022
https://doi.org/10.1016/j.joms.2004.03.0...
,2020. Gupta B, Ponniah I. The pattern of odontogenic tumors in a government teaching hospital in the southern Indian state of Tamil Nadu. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010;110(11):e32-9. doi:10.1016/j.tripleo.2010.02.035
https://doi.org/10.1016/j.tripleo.2010.0...
to be the most common tumor, whereas odontoma has been more frequent in others2121. Ochsenius G, Ortega A, Godoy L, Peñafiel C, Escobar E. Odontogenic tumors in Chile: a study of 362 cases. J Oral Pathol Med. 2002;31(7):415-20. doi:10.1034/j.1600-0714.2002.00073.x
https://doi.org/10.1034/j.1600-0714.2002...
,2222. Buchner A, Merrell PW, Carpenter WM. Relative frequency of central odontogenic tumors: a study of 1,088 cases from Northern California and comparison to studies from other parts of the world. J Oral Maxillofac Surg. 2006;64(9):1343-52. doi:10.1016/j.joms.2006.05.019
https://doi.org/10.1016/j.joms.2006.05.0...
. Interestingly, Fregnani et al.55. Fregnani ER, Fillipi RZ, Oliveira CR, Vargas PA, Almeida OP. Odontomas and ameloblastomas: variable prevalences around the world? Oral Oncol. 2002;38(8):807-8. doi:10.1016/S1368-8375(02)00050-7
https://doi.org/10.1016/S1368-8375(02)00...
emphasized that odontoma is more common in colleges and ameloblastoma is more common in hospital. One possible explanation for this observation is that ameloblastoma treatment requires a more extensive surgery under general anesthesia. Thus, there is a difference in the order of odontogenic tumor prevalence when the studies are in colleges or hospitals. In this prospective study, 25 odontogenic tumors were diagnosed over a period of 15 months. There was a slight predominance of odontomas (9 cases). However, KOT and ameloblastoma also occurred frequently, in 8 and 5 cases, respectively.
It is well accepted that the mandible is the bone most commonly affected by JL (mainly in its posterior region). In a study conducted by Núñez-Urrutia et al.99. Nuñez-Urrutia S, Figueiredo R, Gay-Escoda C. Retrospective clinicopathological study of 418 odontogenic cysts. Med Oral Patol Oral Cir Bucal. 2010;15(5):e767-73. doi:10.4317/medoral.15.e767
https://doi.org/10.4317/medoral.15.e767...
, 61.5% of bone lesions occurred in the mandible. Paradental cysts (97.7%) and dentigerous cysts (69.2%) were observed more in the mandible, while radicular cysts were observed more in the maxilla (56.2%). Similarly, our study showed that the mandible was more frequently affected (100 cases, 71.43%), mainly the body region (71 cases). Dentigerous cysts (100%) and residual cysts (66.67%) were more common in the mandible, and radicular cysts (57.9%) were more common in the maxilla.
A lab retrospective study at Thailand University evaluated 590 odontogenic tumors over a period of 34 years. The mandible was the main site for ameloblastoma, complex odontoma, KOT and calcifying cystic odontogenic tumors. However, the maxilla was more affected by compound odontomas and adenomatoid odontogenic tumors2323. Worawongvasu R, Tiensuwan M. Odontogenic tumors in Thailand: a study of 590 Thai patients. J Oral Maxillofac Surg Med Pathol. 2015;27(4):567-76. doi:10.1016/j.ajoms.2014.11.004
https://doi.org/10.1016/j.ajoms.2014.11....
. Similarly, Gupta et al.2020. Gupta B, Ponniah I. The pattern of odontogenic tumors in a government teaching hospital in the southern Indian state of Tamil Nadu. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010;110(11):e32-9. doi:10.1016/j.tripleo.2010.02.035
https://doi.org/10.1016/j.tripleo.2010.0...
observed that ameloblastoma, ameloblastic fibroma and complex odontoma mainly affect the mandible, and compound odontoma and adenomatoid odontogenic tumors mainly the maxilla. In our study, ameloblastoma (5 cases – 100%), KOT (7 out of 8 cases – 87.5%), compound odontoma (4 out of 7 cases – 57.14%), and calcifying cystic odontogenic tumors (2 out of 3 – 66.66%) more frequently occurred in the mandible. In contrast, the maxilla was more frequently affected by complex odontoma (100%, only 2 cases).
An important radiographic feature of KOT is its anterior-posterior growth. Furthermore, many studies using both panoramic and occlusal x-rays data have not reported bone expansion.11. Neyaz Z, Gadodia A, Gamanagatti S, Mukhopadhyay S. Radiographical approach to jaw lesions. Singapore Med J. 2008;49(2):165-76. In contrast, studies using CT have described a slight expansion of both the buccal and lingual cortical bone.2424. Apajalahti S, Hagström J, Lindqvist C, Suomalainen A. Computerized tomography findings and recurrence of keratocystic odontogenic tumor of the mandible and maxillofacial region in a series of 46 patients. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2011;111(3):e29-37. doi:10.1016/j.tripleo.2010.10.010
https://doi.org/10.1016/j.tripleo.2010.1...
,2525. Ariji Y, Morita M, Katsumata A, Sugita Y, Naitoh M, Goto M, et al. Imaging features contributing to the diagnosis of ameloblastomas and keratocystic odontogenic tumours: logistic regression analysis. Dentomaxillofac Radiol. 2011;40(3):133-40. doi:10.1259/dmfr/24726112
https://doi.org/10.1259/dmfr/24726112...
In the present study, there was CT information in 2 out of 8 KOTs, and both cases presented discrete expansion of the mandible. However, the basal cortical bone was not affected. Interestingly, in the other 2 cases (sinus hypoplasia and Stafne’s bone defect), the CT was fundamental for the diagnosis and clinical management. For the former lesion, osseous dysplasia was the main diagnosis hypothesis in the panoramic x-ray, but after CT, it was determined that the maxilla was normal and a reduction of the size of the maxillary sinus was observed (Figure 2). Consequently, biopsy was not indicated. However, in the other case, the Stafne’s bone defect had been hypothesized in the x-ray, and the CT was essential to confirm the hypothesis.
Osseous dysplasia was observed in 16 patients (mean age of 50.4 years, range 28–77), of whom 12 were women (9 Afro-descendants) and 4 men (3 Afro-descendants). MacDonald-Jankowski2626. MacDonald-Jankowski DS. Florid cemento-osseous dysplasia: a systematic review. Dentomaxillofac Radiol. 2003;32(3):141-9. doi:10.1259/dmfr/32988764
https://doi.org/10.1259/dmfr/32988764...
previously conducted a systematic review of 158 cases of florid osseous dysplasia. The author found that 95% of the cases occurred in Afro-descendants and that 97% in middle-aged women. In a Brazilian retrospective study, a total of 143 fibro-osseous lesions were diagnosed over a period of 9 years. The focal OD were predominantly radiopaque, whereas florid/periapical OD were predominantly mixed.1313. Santos Netto JN, Cerri JM, Miranda AMM, Pires FR. Benign fibro-osseous lesions: clinicopathologic features from 143 cases diagnosed in an oral diagnosis setting. Oral Surg Oral Med Oral Pathol Oral Radiol. 2013;115(5):e56-65. doi:10.1016/j.oooo.2012.05.022
https://doi.org/10.1016/j.oooo.2012.05.0...
In our study, panoramic x-ray was used to diagnosis all of the cases of OD. In all of the cases, the diagnosis was only clinical and radiographic. Of the 11 cases of florid OD, 8 only affected the mandible while 3 affected both the mandible and the maxilla. The other OD cases affected only the mandible. Previous studies also showed that the mandible was more involved than the maxilla.1111. Macdonald-Jankowski DS. Focal cemento-osseous dysplasia: a systematic review. Dentomaxillofac Radiol. 2008;37(6):350-60. doi:10.1259/dmfr/31641295
https://doi.org/10.1259/dmfr/31641295...
,2626. MacDonald-Jankowski DS. Florid cemento-osseous dysplasia: a systematic review. Dentomaxillofac Radiol. 2003;32(3):141-9. doi:10.1259/dmfr/32988764
https://doi.org/10.1259/dmfr/32988764...
In addition, most of the cases were discovered as incidental findings (i.e., there were no symptoms, and biopsy was unnecessary).
Malignancies of the jaw are infrequent. Of the 140 cases diagnosed in this study, only 3 were malignant tumors (osteosarcoma, multiple myeloma and MEC). The osteosarcoma presented as a poorly defined radiopaque image, which caused enlargement of the periodontal ligament and root resorption (panoramic x-ray). Furthermore, the occlusal x-ray showed a “sunburst” pattern. The multiple myeloma was a multilocular radiolucent lesion with disruption of the cortical bone. The other case was a MEC of the maxillary sinus, and the lesion was radiolucent, unilocular, and caused root resorption.
In conclusion, JL are common and represented approximately 30% of all new cases diagnosed at CDO-FOUSP. The main diagnosed lesions were periapical cyst, osseous dysplasia, dentigerous cyst and simple bone cyst. The most common radiographic features observed were radiolucent and unilocular. Biopsy was indicated for 66% of the cases. In the other cases, the diagnosis was concluded through clinical and radiographic features and surgical intervention (only for simple bone cysts).
Acknowledgments
The authors are grateful to the Brazilian Federal Agency for the Support and Evaluation of Graduate Education – CAPES and the National Council for Scientific and Technological Development – CNPq for their financial support. Dr. Fabio Alves is a CNPq research fellow.
References
-
1Neyaz Z, Gadodia A, Gamanagatti S, Mukhopadhyay S. Radiographical approach to jaw lesions. Singapore Med J. 2008;49(2):165-76.
-
2Arotiba JT, Ogunbiyi JO, Obiechina AE. Odontogenic tumours: a 15-year review from Ibadan, Nigeria. Br J Oral Maxillofac Surg. 1997;35(5):363-7. doi: 10.1016/S0266-4356(97)90411-3
» https://doi.org/10.1016/S0266-4356(97)90411-3 -
3Adebayo ET, Ajike SO, Adekeye EO. A review of odontogenic tumors in Kaduna, Nigeria. J Oral Maxillof Surg. 2005;63(6):811-9. doi:10.1016/j.joms.2004.03.022
» https://doi.org/10.1016/j.joms.2004.03.022 -
4Costa DOP, Maurício AS, Faria PAS, Silva LE, Mosqueda-Taylor A, Lourenço SQC. Odontogenic tumors: A retrospective study of four Brazilian diagnostic pathology center. Med Oral Patol Oral Cir Bucal. 2012;17(3):e389-94. doi:10.4317/medoral.17630
» https://doi.org/10.4317/medoral.17630 -
5Fregnani ER, Fillipi RZ, Oliveira CR, Vargas PA, Almeida OP. Odontomas and ameloblastomas: variable prevalences around the world? Oral Oncol. 2002;38(8):807-8. doi:10.1016/S1368-8375(02)00050-7
» https://doi.org/10.1016/S1368-8375(02)00050-7 -
6Kramer IRH, Pindborg JJ, Shear M. Histological typing of odontogenic tumours. 2nd ed. Berlin: Springer; 1992.
-
7Barnes L, Eveson JW, Reichart P, Sidransky D, editors. Pathology and genetics: head and neck tumours. Lyon: IARC Press; 2005. Chapter 6, Odontogenic tumours; p. 283-328. (World Health Organization classification of tumours).
-
8Mosqueda-Taylor A. New findings and controversies in odontogenic tumors. Med Oral Patol Oral Cir Bucal. 2008;13(9):E555-8.
-
9Nuñez-Urrutia S, Figueiredo R, Gay-Escoda C. Retrospective clinicopathological study of 418 odontogenic cysts. Med Oral Patol Oral Cir Bucal. 2010;15(5):e767-73. doi:10.4317/medoral.15.e767
» https://doi.org/10.4317/medoral.15.e767 -
10Avelar RL, Primo BT, Pinheiro-Nogueira CB, Studart-Soares EC, Oliveira RB, Romulo de Medeiros J et al. Worldwide incidence of odontogenic tumors. J Craniofac Surg. 2011;22(6):2118-23. doi:10.1097/SCS.0b013e3182323cc7
» https://doi.org/10.1097/SCS.0b013e3182323cc7 -
11Macdonald-Jankowski DS. Focal cemento-osseous dysplasia: a systematic review. Dentomaxillofac Radiol. 2008;37(6):350-60. doi:10.1259/dmfr/31641295
» https://doi.org/10.1259/dmfr/31641295 -
12Worawongvasu R, Songkampol K. Fibro-osseous lesions of the jaws an analysis of 122 cases in Thailand. J Oral Pathol Med. 2010;39(9):703-8. doi:10.1111/j.1600-0714.2010.00932.x
» https://doi.org/10.1111/j.1600-0714.2010.00932.x -
13Santos Netto JN, Cerri JM, Miranda AMM, Pires FR. Benign fibro-osseous lesions: clinicopathologic features from 143 cases diagnosed in an oral diagnosis setting. Oral Surg Oral Med Oral Pathol Oral Radiol. 2013;115(5):e56-65. doi:10.1016/j.oooo.2012.05.022
» https://doi.org/10.1016/j.oooo.2012.05.022 -
14Perez DEC, Pires FR, Lopes MA, Almeida OP, Kowalski LP. Adenoid cystic carcinoma and mucoepidermoid carcinoma of the maxillary sinus: report of a 44-year experience of 25 cases from a single institution. J Oral Maxillofac Surg. 2006;64(11):1592-7. doi:10.1016/j.joms.2005.11.088
» https://doi.org/10.1016/j.joms.2005.11.088 -
15Bachar G, Goldstein D, Brown D, Tsang R, Lockwood G, Perez-Ordonez B et al. Solitary extramedullary plasmacytoma of the head and neck: long-term outcome analysis of 68 cases. Head Neck. 2008;3098):1012-9. doi:10.1002/hed.20821
» https://doi.org/10.1002/hed.20821 -
16Kamal M, Kaur P, Gupta R, Gupta S, Singh S. Mandibular plasmacytoma of jaw: a case report. J Clin Diagn Res. 2014;8(8):ZD20-1. doi:10.7860/JCDR/2014/9565.4674
» https://doi.org/10.7860/JCDR/2014/9565.4674 -
17Stewart BD, Reith JD, Knapik JA, Chi AC. Bone and cartilage-forming tumors and ewing sarcoma: an update with a gnathic emphasis. Head Neck Pathol. 2014;8(4):454-62. doi:10.1007/s12105-014-0587-8
» https://doi.org/10.1007/s12105-014-0587-8 -
18Marx RE. Osteoradionecrosis: a new concept of its pathophysiology. J Oral Maxillofac Surg. 1983;41(5):283-8. doi:10.1016/0278-2391(83)90294-X
» https://doi.org/10.1016/0278-2391(83)90294-X -
19Daley TD, Wysocki GP, Pringle GA. Relative incidence of odontogenic tumors and oral and jaw cysts in a Canadian population. Oral Surg Oral Med Oral Pathol. 1994;77(3):276-80. doi:10.1016/0030-4220(94)90299-2
» https://doi.org/10.1016/0030-4220(94)90299-2 -
20Gupta B, Ponniah I. The pattern of odontogenic tumors in a government teaching hospital in the southern Indian state of Tamil Nadu. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010;110(11):e32-9. doi:10.1016/j.tripleo.2010.02.035
» https://doi.org/10.1016/j.tripleo.2010.02.035 -
21Ochsenius G, Ortega A, Godoy L, Peñafiel C, Escobar E. Odontogenic tumors in Chile: a study of 362 cases. J Oral Pathol Med. 2002;31(7):415-20. doi:10.1034/j.1600-0714.2002.00073.x
» https://doi.org/10.1034/j.1600-0714.2002.00073.x -
22Buchner A, Merrell PW, Carpenter WM. Relative frequency of central odontogenic tumors: a study of 1,088 cases from Northern California and comparison to studies from other parts of the world. J Oral Maxillofac Surg. 2006;64(9):1343-52. doi:10.1016/j.joms.2006.05.019
» https://doi.org/10.1016/j.joms.2006.05.019 -
23Worawongvasu R, Tiensuwan M. Odontogenic tumors in Thailand: a study of 590 Thai patients. J Oral Maxillofac Surg Med Pathol. 2015;27(4):567-76. doi:10.1016/j.ajoms.2014.11.004
» https://doi.org/10.1016/j.ajoms.2014.11.004 -
24Apajalahti S, Hagström J, Lindqvist C, Suomalainen A. Computerized tomography findings and recurrence of keratocystic odontogenic tumor of the mandible and maxillofacial region in a series of 46 patients. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2011;111(3):e29-37. doi:10.1016/j.tripleo.2010.10.010
» https://doi.org/10.1016/j.tripleo.2010.10.010 -
25Ariji Y, Morita M, Katsumata A, Sugita Y, Naitoh M, Goto M, et al. Imaging features contributing to the diagnosis of ameloblastomas and keratocystic odontogenic tumours: logistic regression analysis. Dentomaxillofac Radiol. 2011;40(3):133-40. doi:10.1259/dmfr/24726112
» https://doi.org/10.1259/dmfr/24726112 -
26MacDonald-Jankowski DS. Florid cemento-osseous dysplasia: a systematic review. Dentomaxillofac Radiol. 2003;32(3):141-9. doi:10.1259/dmfr/32988764
» https://doi.org/10.1259/dmfr/32988764
Publication Dates
-
Publication in this collection
2016
History
-
Received
30 Nov 2015 -
Reviewed
23 May 2016 -
Accepted
08 June 2016