
Abstract
Objectives:
this study aims to evaluate parturition distribution of live-born children within the First Health Regional Administration (GERES I) in the state of Pernambuco, Brazil in 2012.
Methods:
live Birth Certificates were used to evaluate displacements between pregnant women's residential municipalities and birth localities. Flux maps were constructed to represent pregnant women transferred to Recife, and the estimated number of live-borns with high-risk and regular births was calculated for each municipality.
Results:
in 2012, only 50% of the births of live babies in the GERES I took place at the original residential municipality of the mother. In Recife, the number of childbirths was 1.5 times greater than expected for this year, with 56% representing non-residents. Eleven municipalities of the GERES I have maternity hospitals, however, none of these responded to the expected number of regular risk births.
Conclusions:
this disruption of the obstetric network leads to the disrespecting of women's right to know beforehand the place of childbirth and to create bonds with it. Municipalities perform fewer childbirths than expected, resulting in unnecessary transfers and the overloading of maternity hospitals in Recife.
Key words:
Birth; Regional health planning; Health services accessibility; Residence characteristics
Resumo
Objetivos:
saber o local onde irá ocorrer o parto é um direito da gestante no Brasil e uma estratégia de organização da rede de atenção obstétrica. Este estudo tem como objetivo avaliar a distribuição dos partos dos nascidos vivos (NV) da Gerência Regional de Saúde (GERES) I do Estado de Pernambuco em 2012.
Métodos:
a partir das Declarações de Nascidos Vivos, foram investigados deslocamentos do município de residência da mãe e de ocorrência do parto. Foram construídos mapas de fluxo para o Recife e estimado o número esperado de NV com parto de risco habitual e de alto risco para os municípios da GERES I.
Resultados:
em 2012 apenas 50% dos NV da GERES I nasceram no município de residência da mãe. Em Recife ocorreram 1,5 vezes o número de partos esperados para o ano, sendo 56% de mães não residentes. Onze municípios da GERES I têm maternidade, mas nenhum responde ao volume esperado de partos de risco habitual.
Conclusões:
esta desestruturação da rede obstétrica viola o direito da mulher de saber com antecedência e construir vínculo com o local do parto. Alguns municípios da GERES I realizam menos partos do que o esperado, levando a transferências desnecessárias e a super-lotação das maternidades do Recife.
Palavras-chave:
Assistência ao parto; Regionalização; Acesso aos serviços de saúde; Distribuição espacial da população
Introduction
A strategy to improve the distribution of childbirths in the territory is decentralization, which is defined by the Public Health System (SUS) guidelines. It is a right ensured by law that pregnant women should know where their delivery will occur, in order to create bonding during the prenatal care with the obstetrics service, where the delivery will occur.11 Brasil. Lei nº 11.634, de 27 de dezembro de 2007. Sobre o direito da gestante ao conhecimento e vinculação à maternidade onde receberá assistência no âmbito do Sistema Único de Saúde. Diário Oficial da União 28 dez 2007; Seção 1.
The location for childbirth care should be structured by decentralization. In Brazil, these initiatives are quite recent, configuring disparities between the coverage of prenatal care and the system for child-birth and birth care, which are still insufficient for the demand. In the absence of an effective regionalized system, a disordered flow of pregnant women occurs in search for a safe place for delivery.22 Cunha SF, Júnior ADE, Rios CTF, Pestana AL, Mochel EG, Paiva SS. Peregrinação no anteparto em São Luís - Maranhão. Cogitare Enferm. 2010; 15 (3): 441-47.
In defining the obstetric care system, it is the responsibility of the city, by means of basic care, to ensure prenatal care and low risk childbirth, assuring that high risk pregnant women go to appropriate referral complexity units to be attended at the service. Thus, the district plays a vital role in maintaining the system as an integrated system. The demand for the high risk is restricted to specialized services that incorporate more technology.33 Santos MAS, Cruz JB, Silva VR. Desafios da regionalização da assistência à gestante e ao parto na V GERES, Garanhuns, Pernambuco. Journal of Management and Primary Health Care. 2011; 2 (2): 11-4.
The regionalized obstetric care network should guide the process of decentralization and to integrate health services and actions. The regionalization should be the axis structure management, as defined by the Pact for Life (Pacto pela Vida), in defense of SUS and the Management.4 In this model, each health regional district should be self-sufficient at least until the average complexity by the processes of negotiation and until the medium complexity agreement among managers. The Mother Owl Program (Programa Mãe Coruja) was founded to reduce maternal and infant morbimortality in the State, provided for (re)structuring the obstetric care in each Regional Management Health District (GERES). These are grouped into four macro regions, that should internally respond to the entire high risk demand of resident pregnant women,5 consequently reducing the displacements for childbirth.
The ideal location for childbirth is the one chosen by the pregnant woman, where she feels safe and to which she can build a bond during her pregnancy. The low risk pregnant women should preferably give birth in service nearby to their residence, allowing partners, family and friends to accompany them, avoiding risks of distant travels to far away services.11 Brasil. Lei nº 11.634, de 27 de dezembro de 2007. Sobre o direito da gestante ao conhecimento e vinculação à maternidade onde receberá assistência no âmbito do Sistema Único de Saúde. Diário Oficial da União 28 dez 2007; Seção 1.
As a strategy to reduce unnecessary displacements and organize the flow of pregnant women to available services closer to their homes according to the required complexity level, the Central Regulation for Hospital Beds was founded. This strategy integrates the obstetric care management in Pernambuco State and regulates pregnant women throughout the territory.66 Pernambuco. Secretaria Estadual de Saúde. Manual Operacional - Central de Regulação de Leitos. Recife, PE; 2014.
In 2011, the Ministry of Health released a strategy called the Stork System (Rede Cegonha), aiming to improve care for women and their newborns, founded on the principle of humanized care. It is proposed to extend the access, hospitality and quality of prenatal care improvement, bonding pregnant woman to a reference unit for childbirth care, performing safe childbirth and delivery through good practices.77 Brasil. Ministério da Saúde. Portaria nº 1.459, de 24 de junho de 2011. Institui - no âmbito do Sistema Único de Saúde - SUS - a Rede Cegonha. Diário Oficial da União 27 jun 2011; Seção 1. However, in Pernambuco, the system is still in implementation process.
The Stork System follows the logic of localization88 Brasil. Ministério da Saúde. Portaria n° 650, de 05 de outubro de 2011. Dispõe sobre os Planos de Ação regional e municipal da Rede Cegonha. Diário Oficial da União 6 out 2011; Seção 1. in Pernambuco State. Recife is the capital of the State and is the main area of the Macro Regional I which concentrates the high risk obstetrics hospitals of the region. Thus, Recife city should receive high risk pregnant women (estimated by the World Health Organization in 15% of all pregnancies) from the districts of GERES I, II, III and XII, which compose the Macro Regional and also should perform childbirths of low risk pregnant women.
The objective of this study is to describe the distribution of deliveries of live births from GERES I in Pernambuco State in 2012 and the displacements made by pregnant women at the time of the delivery. The hypothesis is that the overcrowding of obstetrical services in Recife is caused not only by the transference of high risk pregnant women from other districts of the Macro Regional, but mainly by low risk pregnant women inappropriately refered from maternity hospitals from GERES I, which leads these women to give birth in Recife city.
Methods
This is an ecological population based study, that takes the cities as the analysis unit. The information was collected from the Live Births Certificates (DNV), of women living in Pernambuco, registered in the Information System on Live Births (SINASC) with births from 01/01/2012 to 12/31/2012. The study area was the Health Macro Regional I which includes Health Management of Regional Districts (GERES) I, II, III and XII in the State. The study population was composed by all women who resided in the study area which had live births during the period described. The location of the mother´s residence and of the occurrence of childbirth were investigated. The NVs' mothers residing in the city of GERES I were categorized as born in the city of residency or outside of it.
The ability to conduct childbirths by the cities was defined by the number of deliveries that were actually performed, regardless of the women's location of residency. It was also calculated the number of NVs with high and low risk from each city, whereas the parameters were of 15% and 85% of the total number, respectively.8 For this calculation, it was taken in consideration of NVs' mothers residing in that minucipality, regardless of the city where the birth occurred. For each city of GERES I, except for Recife city, the chisquare test was applied to assess whether there was a significant difference between the number estimated of high risk newborns and the number of newborns born in Recife.
To demonstrate the displacements of pregnant women from their cities of residency to the location of birth, displacement flow maps were created by ArcGIS 9.3 program. The flow maps represent the movement of people in space, showing the direction and the magnitude of the studied movement by means of vectors drawn on the itinerary taken.9 In this study, the flow was characterized quantitatively by means of thick proportions, permitting the identification of the traffic volume in between the city of residency and the place of birth. Only the origin and the final destination were used since the intermediate course was not possible to be verified with the SINASC data, but only the origin and the final destination were used.
Two maps were made; the first represented the displacements that occurred from the cities of residency to the place of birth. The second compares the volume of deliveries that actually happened with the number expected to occur in Recife city - the main reference for high risk in Macro Regional I which would receive the high risk (15%) NVs of mothers living in other cities.
The districts identified with more than 300 low risk NVs of residing mothers in the year were considered as appropriate for the existence of services of childbirth care. According to international criteria, the existence of services that perform below 300 births per year is not justified in financial and operational terms, except in localities with very difficult access.1010 Schramm JMA, Szwarcwald CL, Esteves MAP. Assistência obstétrica e risco de internação na rede de hospitais do Estado do Rio de Janeiro. Rev Saúde Pública. 2002; 36 (5): 590-7.
Results
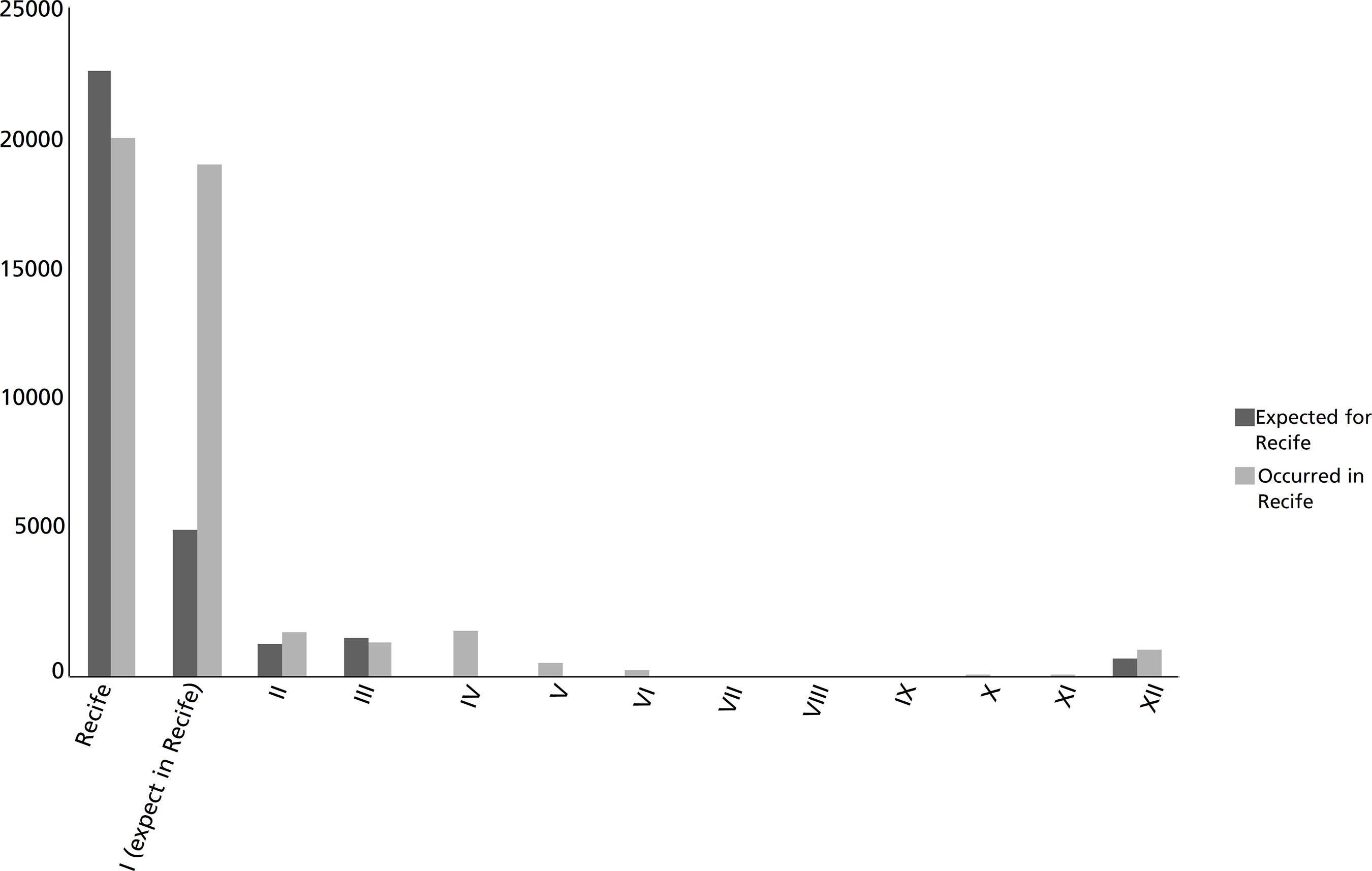
In the studied year, 46,072 NV were born in Recife, from which 20,126 (44%) born by mothers who lived in Recife. The actually expected number was 31,606 (summed the high from the Macro Regional I and low risk from residents in Recife). On the other hand, from the total of 22,641 NV of women living in Recife, 2,515 (11%) occurred outside the city. Of the total number of deliveries of NVs in Recife, 62% (28,558) were from SUS. Figure 1 shows the number of NVs' births occurred and expected in Recife according to GERES of mothers who lived in Pernambuco.
Number of live births expected and occurred in Recife by GERES of mothers’ residency, 2012.
In 2012, Recife city responded to 88.9% of the demand for deliveries of live births of mothers living in the Recife. The deliveries of women from Recife occurred outside the city, 95% (2,386) were in SUS maternity hospitals. Most were sent to health units located in Olinda or Jaboatão dos Guararapes. Olinda received 4.7% of the NVs of mothers living in Recife and Jaboatão dos Guararapes, 3%. The other cities of GERES I received 3%, while 0.6% were born outside GERES or the State.
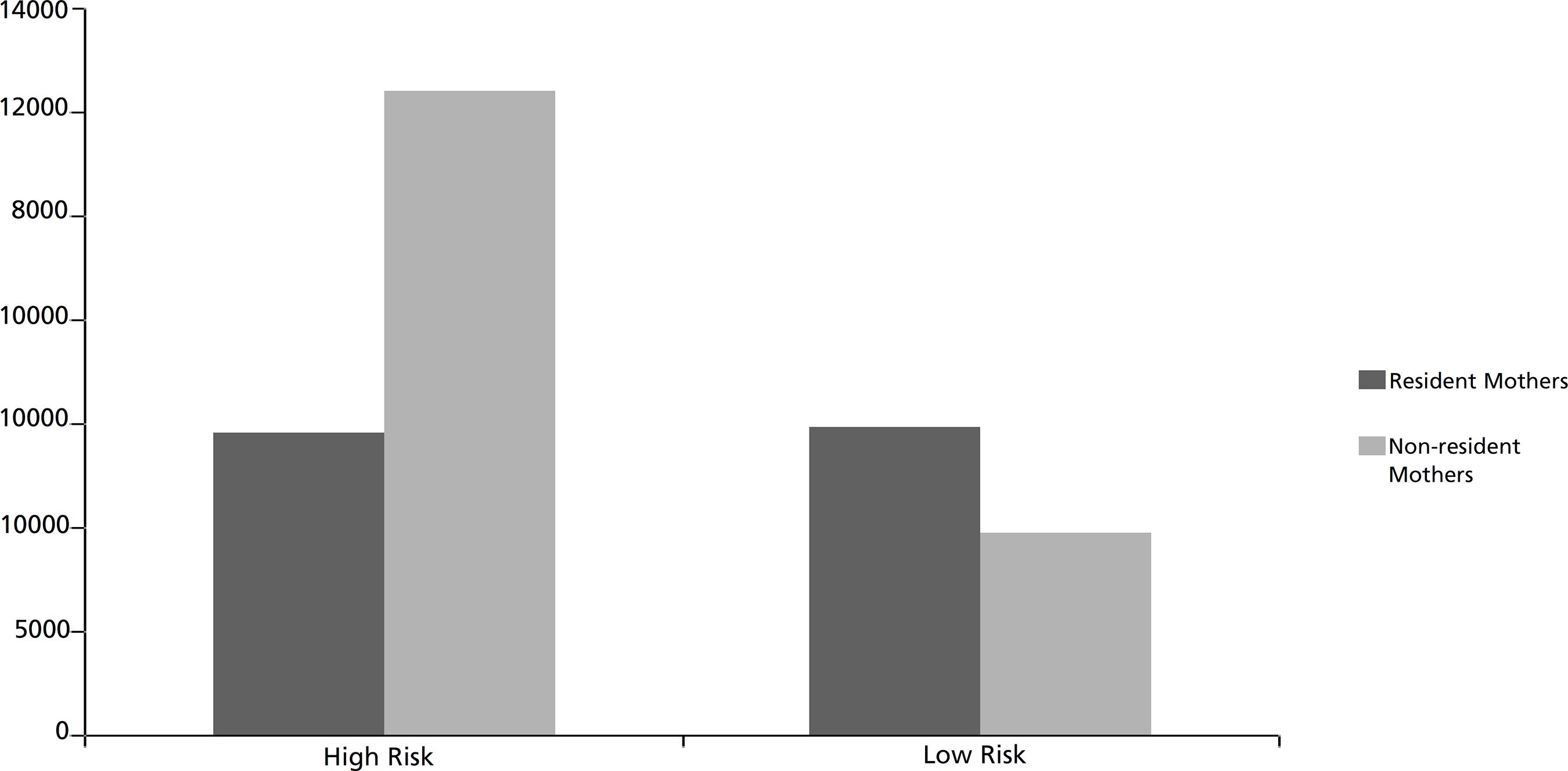
Of the 59,479 live births registered in SINASC of mothers living in GERES I, only 50% (29,712) of the children were born in the cities where their mothers lived. Whereas the expected number for high risk corresponded to 15% ,8 estimated at 8,921 live births of high risk pregnancy and 55,557 of low risk. Among the NVs from SUS system, the volume of births exceeded of what would be expected based on the risk criteria (Figure 2).
Number of live births occurred in services with high and low risk pregnancy at SUS of mother residents and non-residents in Recife, 2012.
Of the 20 cities in GERES I, nine had less than 300 NV of resident mothers living in: Igarassu, Glória do Goitá, Pombos, Itapissuma, Araçoiaba, Chã Grande, Ilha de Itamaracá, Chã de Alegria and Fernando de Noronha. For all of these locations, except Igarassu, the expected number of NV from mothers resident of these locations was also less than 300 Nvs.
The city of Igarassu had 1,516 NV of resident mothers, from which 1,289 were estimated of low risk. But only 31 deliveries occurred in the city in 2012, from which 25 were resident mothers. Jaboatão dos Guararapes, Olinda, Paulista, Cabo de Santo Agostinho, Camaragibe, Vitória de Santo Antão, Ipojuca, São Lourenço da Mata, Abreu e Lima and Moreno have maternity units for low risk pregnancy. However, none of these cities reached 85% of the number estimated of low risk live births of mothers living in this municipality, even though some demonstrate the capacity to perform a number higher than expected (Figure 3).
Number of live births of low risk pregnancy expected in each city of mother residency, number of live births occurred in each city of mother residency and the total number of live births by cities in GERES I. Pernambuco, 2012.
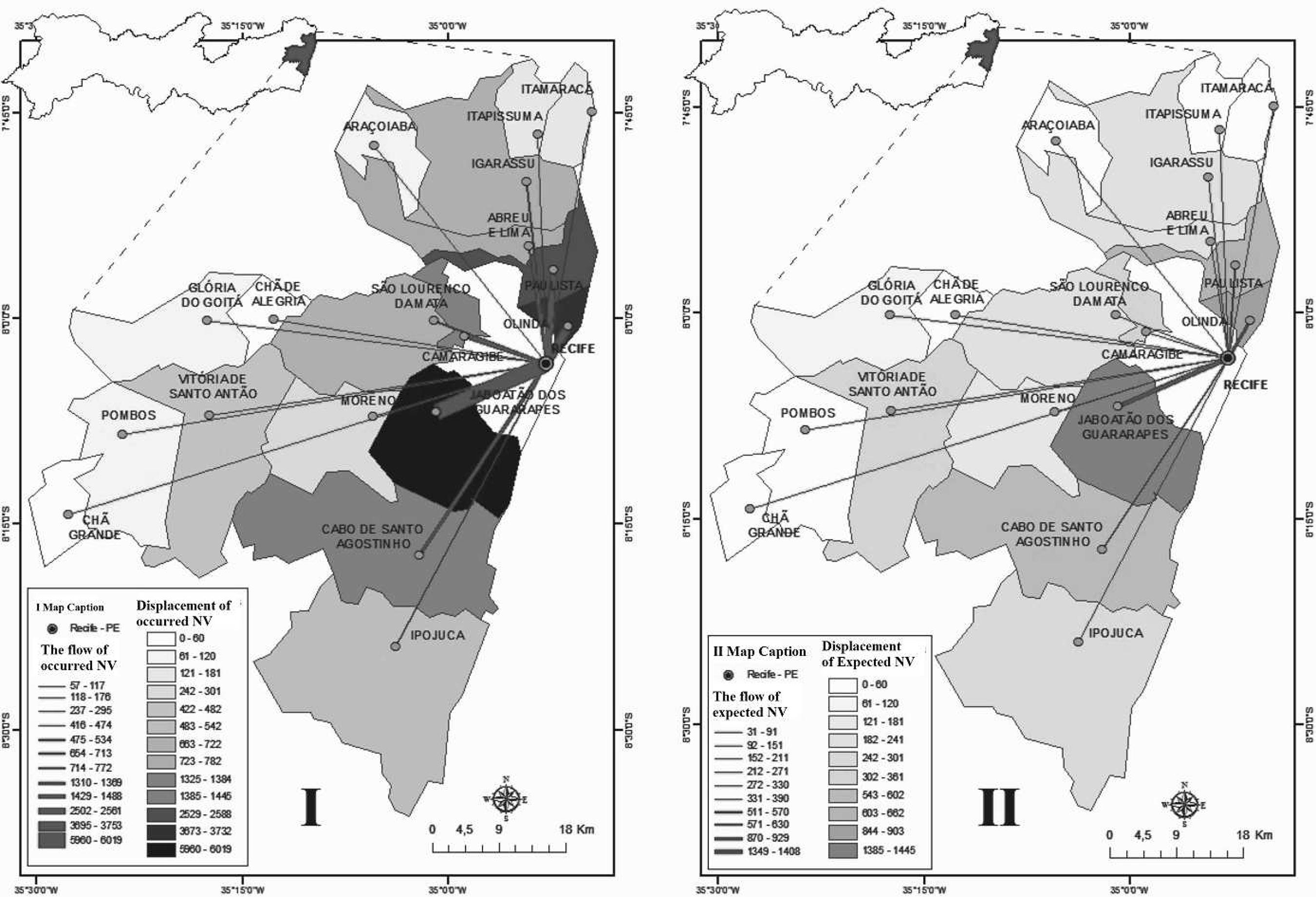
The flow maps (Figure 4) NV the displacement of pregnant women living in the cities of GERES I to Recife city. Map II shows the displacements expected of high risk (15% of the NV of mothers residing in each city). The number of NV in Recife of mothers living in GERES I, excluding Recife, was significantly higher than expected for high risk pregnancy, except for Pombos and Chã de Alegria (Table 1).
Map I: Displacement of mothers in GERES I to Recife city, the location where the live births occurred. Pernambuco, 2012. Map II: Expected Displacements of high risk pregnancy (15% of the NV of mothers residing in each city in GERES I). Pernambuco, 2012.
Number of live births occurred in Recife city and the number of live births of high risk pregnancy estimated by the cities of GERES I, with the value of p, by city of the mother's residency. Pernambuco, 2012.
Discussion
In 2012, occurred in Recife 46% more deliveries than expected for the city as the center of the Macro Regional I. On the other hand, only 89% of NV deliveries of mothers resident in Recife happened in the city. Still, Recife city received 43% of the total low risk pregnancy women from the GERES I, which should have been attended in their cities of residency. Recife also received women from other Health Macro Regional of the State. Among the 12 cities with number of live births that justified the existence of obstetric care service, only one city did not have one. Despite having their own services that perform childbirths in greater number than expected for low risk pregnancy, none of them responded to their own demand.
One of the limitations of the present study is the displacement analysis contemplated only to the place of residency and the location where the delivery occurred, not allowing to identify the difficulties in having access to maternity hospitals and the peregrination of women to the place of the delivery. A study conducted in 2013 to assess the displacement of women from Pernambuco, by interviewing 618 puerperal women residing in 123 municipalities with high risk delivery in maternity hospitals in Recife, showed that half of the women studied had to seek assistance in two maternity hospitals to be effectively admitted to a maternity; 11.5% sought for assistance in three or more maternity hospitals.1111 Pinheiro HDM. Do domicilio ao parto: avaliação do acesso às maternidades de alto risco da cidade do Recife - PE [dissertação]. Recife: Programa de Pós-graduação Integrado em Saúde Coletiva da Universidade Federal de Pernambuco; 2014. A Brazilian survey 12 held between 2011 -2012 documented that the displacement at the moment of hospitalization for the delivery was more frequent among women residing in the Northeast region of the country.
The obstetric care system of the Macro Regional I should offer childbirth services to women who reside in this location, adequate for the complexity level of the delivery and the proximity to the location of the women's residency. The establishment of health care network improves the quality of the services, the health worker's and user's satisfaction, of the users, as well as reduces costs with the health-care system.1313 Mendes EV. As redes de atenção à saúde. Ciência & Saúde Coletiva. 2010; 15 (5): 2297-2305. The definition of integrated systems establishes that primary care services, which should be the main location for prenatal care, coordinate the flow of care,1414 Cecilio LCO, Andreazza R, Carapinheiro G, Araújo EC, Oliveira LA, Andrade MGG, Meneses CS, Pinto NRS, Reis DO, Santiago S, Souza ALM, Spedo AM. A Atenção Básica à Saúde e a construção das redes temáticas de saúde: qual pode ser o seu papel? Ciênc Saúde Coletiva. 2012; 17 (11): 2893 -2902. defining reference and counterreference systems to ensure completeness..
In the organizational model proposed for SUS in Recife, the low risk delivery should occur in maternity hospitals in the city area. Nevertheless, 40% of the deliveries that happened in low risk birth facilities in Recife were from non-resident women, which is evidentially not a responsability of the city of Recife. Paradoxically, the system did not assist women resident of the city with low risk deliveries, so they were displaced to a high complexity service or had to be attended elsewhere. This inadequacy in the referencing, leads to unnecessary overcrowding in the maternity hospitals in Recife, especially those of high risk pregnancy that should be exclusive for more complex cases.
It would be more appropriate to transfer to Recife only high risk pregnant women residents in the 19 cities in GERES I, however, the number attended was three times higher than expected for the high risk pregnancies. Such transferences would be acceptable only for the eight cities with the expected number of births which does not justify the existence of obstetric care service.1010 Schramm JMA, Szwarcwald CL, Esteves MAP. Assistência obstétrica e risco de internação na rede de hospitais do Estado do Rio de Janeiro. Rev Saúde Pública. 2002; 36 (5): 590-7.
The fact that half of the GERES I had their children outside the district of residency, evidences the disruption of the system. In addition, women from other Health Macro Regions had their deliveries in Recife city, what should have not occurred, since each Macro Regional is responsable for the totality of its births. In 2013, a survey was carried out in Recife showing that eighty per cent of the puerperal women interviewed did not have their deliveries in the maternity hospital that were indicated during their prenatal care.1111 Pinheiro HDM. Do domicilio ao parto: avaliação do acesso às maternidades de alto risco da cidade do Recife - PE [dissertação]. Recife: Programa de Pós-graduação Integrado em Saúde Coletiva da Universidade Federal de Pernambuco; 2014.
Standards established by the Regulation Center os Hospital Beds in the State of Pernambuco admits the transference of low risk pregnant women to another unit in the same level of complexity or to high risk care units, when there is the "lack of equipment or incomplete team."66 Pernambuco. Secretaria Estadual de Saúde. Manual Operacional - Central de Regulação de Leitos. Recife, PE; 2014. It is possible that the volume of deliveries of low risk pregnancy conducted in the unit with inadequate complexity is the result of the precarious SUS network.1515 Assunção MF, Soares RC, Serrano I. A Superlotação das Maternidades em Pernambuco no contexto atual da Política de Saúde. Serviço Social em Revista. 2014; 16(2): 05-35. The innumerous situations that lead to restriction for admission to childbirth services cause the underutilization of obstetric beds for low risk pregnancy and unnecessary public spending for maintenance of services that do not use all their capacity. On the other hand, services that are working normally are overcrowded, with low quality of care and displacing women in search of a place to give birth.33 Santos MAS, Cruz JB, Silva VR. Desafios da regionalização da assistência à gestante e ao parto na V GERES, Garanhuns, Pernambuco. Journal of Management and Primary Health Care. 2011; 2 (2): 11-4. The restriction of services for high risk pregnancy can be established only in exceptional situations.66 Pernambuco. Secretaria Estadual de Saúde. Manual Operacional - Central de Regulação de Leitos. Recife, PE; 2014.
An effective system to regulate and referencing, as well as clinical protocols for risk assessment would reduce this distortion in the access to the services.1616 Menezes DCS, Leite IC, Schramm JMA, Leal MC. Avaliação da peregrinação anteparto numa amostra de puérperas no Município do Rio de Janeiro, Brasil, 1999/2001. Cad Saúde Pública. 2006; 22 (3): 553-9.
One of the ways to reduce the overcrowding of childbirth services in Recife is to ensure the continued service at the maternity hospitals for low risk pregnancy in all GERES I. The transference of low risk pregnant women usually justifies only for the municipalities with less than 300 NV of residet mothers per year. It would be recommended the establishment of a maternity hospital for low risk pregnancy in the district of Igarassu, because the existing demand overloads the services from other districts, especially in Recife. Through the study of the flow of the service users, it is possible to identify the problems of access in areas with few services, decentralization opportunities and alternatives for regionalization,99 Melo ECP, Knupp VMAO, Oliveira RB, Tonini T. A peregrinação das gestantes no Município do Rio de Janeiro: perfil de óbitos e nascimentos. Revista da Escola de Enfermagem da USP. 2007; 41: 804-9. and evidenced situations which were identified in the studied area.
The findings showed that the bond of the pregnant women with the nearby services of their residence were secondary. A study carried out in Rio de Janeiro pointed out that the satisfaction assessment of women in relation to the attendance at the delivery was associated mainly to get a place to stay at the hospital.1717 Dias MAB, Deslandes SF. Expectativas sobre a assistência ao parto de mulheres usuárias de uma maternidade pública do Rio de Janeiro, Brasil: os desafios de uma política pública de humanização da assistência. Cad Saúde Pública. 2006; 22 (12): 2647-55. To know where the delivery will occur, besides being a right in Brazilian law, is a way to give more tranquility to the pregnant woman. The creation of a bond between the pregnant women and the childbirth care service during their prenatal care also increases the social demand that the city takes responsibility in ensuring the delivery care for the low risk pregnancies of its residents.22 Cunha SF, Júnior ADE, Rios CTF, Pestana AL, Mochel EG, Paiva SS. Peregrinação no anteparto em São Luís - Maranhão. Cogitare Enferm. 2010; 15 (3): 441-47.
According to Mendes, 13 the health care system should be organized as a polyarchy of health services with a unique mission, common goals and a cooperative and interdependent action. Thus, offering a continuous and integral care, providing safe and timely location, with suitable cost in a qualified and humanized form.1313 Mendes EV. As redes de atenção à saúde. Ciência & Saúde Coletiva. 2010; 15 (5): 2297-2305. The effective implementaion of the regionalized obstetric care system in the studied area is necessary and can be achieved through the strengthening of deals among municipality managers, a better distribution of the obstetric care services and a more efficient system of referencing for the nearby cities.
The results of this study showed a disruption in the obstetric network system at GERES I in Pernambuco State. This desorganization leads to overcrowding of the maternity hospitals in Recife city, and has as consequence the violation of women's right to know in advance the health service in which her delivery will occur and build bonds to it during pregnancy.
References
-
1Brasil. Lei nº 11.634, de 27 de dezembro de 2007. Sobre o direito da gestante ao conhecimento e vinculação à maternidade onde receberá assistência no âmbito do Sistema Único de Saúde. Diário Oficial da União 28 dez 2007; Seção 1.
-
2Cunha SF, Júnior ADE, Rios CTF, Pestana AL, Mochel EG, Paiva SS. Peregrinação no anteparto em São Luís - Maranhão. Cogitare Enferm. 2010; 15 (3): 441-47.
-
3Santos MAS, Cruz JB, Silva VR. Desafios da regionalização da assistência à gestante e ao parto na V GERES, Garanhuns, Pernambuco. Journal of Management and Primary Health Care. 2011; 2 (2): 11-4.
-
4Brasil. Ministério da Saúde. Diretrizes Operacionais dos Pactos pela Vida, em Defesa do SUS e de Gestão. Brasília, DF; 2006.
-
5Pernambuco. Lei nº 13.959 de 15 de dezembro de 2009. Programa Mãe Coruja Pernambucana. Diário Oficial do Estado de Pernambuco 16 dez 2009; Seção 1.
-
6Pernambuco. Secretaria Estadual de Saúde. Manual Operacional - Central de Regulação de Leitos. Recife, PE; 2014.
-
7Brasil. Ministério da Saúde. Portaria nº 1.459, de 24 de junho de 2011. Institui - no âmbito do Sistema Único de Saúde - SUS - a Rede Cegonha. Diário Oficial da União 27 jun 2011; Seção 1.
-
8Brasil. Ministério da Saúde. Portaria n° 650, de 05 de outubro de 2011. Dispõe sobre os Planos de Ação regional e municipal da Rede Cegonha. Diário Oficial da União 6 out 2011; Seção 1.
-
9Melo ECP, Knupp VMAO, Oliveira RB, Tonini T. A peregrinação das gestantes no Município do Rio de Janeiro: perfil de óbitos e nascimentos. Revista da Escola de Enfermagem da USP. 2007; 41: 804-9.
-
10Schramm JMA, Szwarcwald CL, Esteves MAP. Assistência obstétrica e risco de internação na rede de hospitais do Estado do Rio de Janeiro. Rev Saúde Pública. 2002; 36 (5): 590-7.
-
11Pinheiro HDM. Do domicilio ao parto: avaliação do acesso às maternidades de alto risco da cidade do Recife - PE [dissertação]. Recife: Programa de Pós-graduação Integrado em Saúde Coletiva da Universidade Federal de Pernambuco; 2014.
-
12Viellas EF, Domingues RMSM, Dias MAB, Gama SGN, Theme Filha MM, Costa JV, Bastos MH, Leal MC. Assistência pré-natal no Brasil. Cad Saúde Pública. 2014; 30 (1): S85- S100.
-
13Mendes EV. As redes de atenção à saúde. Ciência & Saúde Coletiva. 2010; 15 (5): 2297-2305.
-
14Cecilio LCO, Andreazza R, Carapinheiro G, Araújo EC, Oliveira LA, Andrade MGG, Meneses CS, Pinto NRS, Reis DO, Santiago S, Souza ALM, Spedo AM. A Atenção Básica à Saúde e a construção das redes temáticas de saúde: qual pode ser o seu papel? Ciênc Saúde Coletiva. 2012; 17 (11): 2893 -2902.
-
15Assunção MF, Soares RC, Serrano I. A Superlotação das Maternidades em Pernambuco no contexto atual da Política de Saúde. Serviço Social em Revista. 2014; 16(2): 05-35.
-
16Menezes DCS, Leite IC, Schramm JMA, Leal MC. Avaliação da peregrinação anteparto numa amostra de puérperas no Município do Rio de Janeiro, Brasil, 1999/2001. Cad Saúde Pública. 2006; 22 (3): 553-9.
-
17Dias MAB, Deslandes SF. Expectativas sobre a assistência ao parto de mulheres usuárias de uma maternidade pública do Rio de Janeiro, Brasil: os desafios de uma política pública de humanização da assistência. Cad Saúde Pública. 2006; 22 (12): 2647-55.
Publication Dates
-
Publication in this collection
Oct-Dec 2016
History
-
Received
28 Jan 2016 -
Reviewed
08 Nov 2016 -
Accepted
21 Dec 2016

 Fonte: SINASC/DATASUS, 2012.
Fonte: SINASC/DATASUS, 2012.
 Fonte: SINASC/DATASUS, 2012.
Fonte: SINASC/DATASUS, 2012.
 Fonte: SINASC/DATASUS, 2012.
Fonte: SINASC/DATASUS, 2012.
 Fonte: SINASC/DATASUS, 2012.
Fonte: SINASC/DATASUS, 2012.