Abstracts
This case report involves a 20-year-old man with unilateral punctate porokeratosis. The patient presented an 8-year history of numerous asymptomatic keratotic papules and pits with linear distribution on his left pal-mar surface and fifth finger of the left hand. Histopathological examination of the keratotic plug revealed findings of distinct epidermal depressions containing cornoid lamellae. This report review draws attention to differential diagnoses of punctate porokeratosis.
Diagnosis; Differential diagnosis; Histology; Porokeratosis
Relata-se o caso de um homem de 20 anos de idade com poroceratose punctata, caracterizada por múltiplas pápulas queratósicas e depressões, com disposição linear localizada à região palmar da mão e 5º dedo esquerdos, com cerca de 8 anos de evolução. O estudo histológico mostrou presença de depressão da epiderme, preenchida por característica lamela cornóide. Foi realizada revisão da literatura e ressaltado o seu diagnóstico diferencial.
Diagnóstico; Diagnóstico diferencial; Histologia; Poroceratose
INTRODUCTION
Since Brown's first description (1971) of "punctate keratoderma", multiple palmo-plantar minute keratotic projections have been described in many different ways, leading to much terminological confusion in the literature.11. Brown FC. Punctate keratoderma. Arch Dermatol. 197;104:682-3. Punctate porokeratotic keratoderma (palmaris et plantaris), spiny keratoderma and punctate porokeratosis (palmaris et plantaris) are frequently referred to indiscriminately as if they referred to the same assumption.22. Herman PS. Punctate porokeratotic keratoderma. Dermatologica. 1973;147:206-13.
3. Osman Y, Daly TJ, Don PC. Spiny keratoderma of the palms and soles. J Am Acad Dermatol. 1992;26:879-81.
-
44. Himmelstein R, Lynfield YL. Punctate porokeratosis. Arch Dermatol. 1984; 120:263-4. More recent publications have however highlighted major distinctions between these descriptions.55. Caccetta TP, Dessauvagie B, McCallum D, Kumarasinghe SP. Multiple minute digitate hyperkeratosis: A proposed algorithm for the digitate keratoses. J Am Acad Dermatol. 2012;67:e49-55.
CASE REPORT
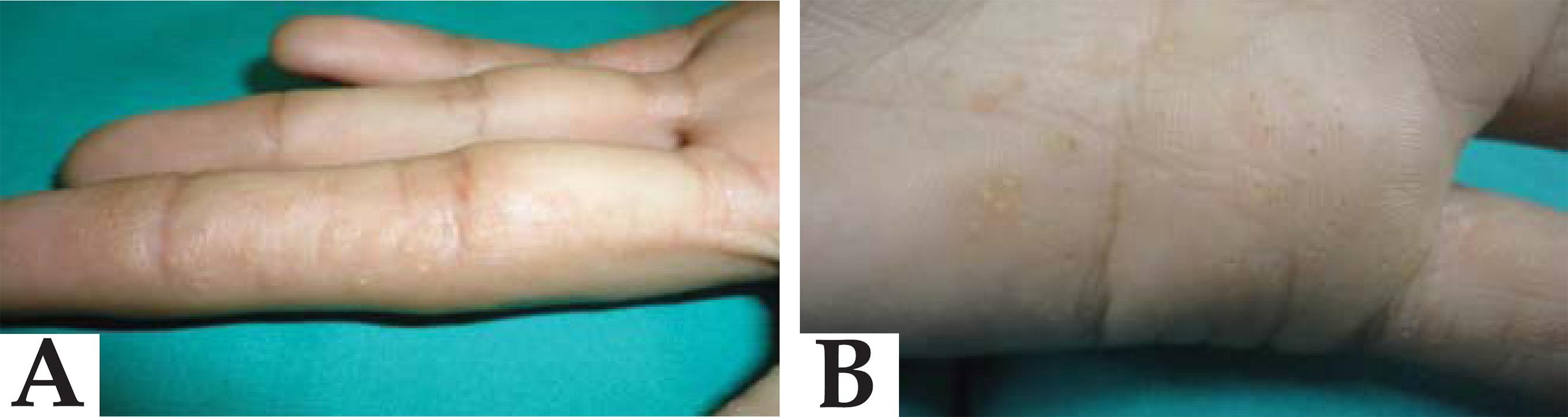
Our case involved a 20-year-old basically healthy adult male with multiple keratotic papules, central keratin plug, 2-3 mm in diameter, located on the left palmar surface of the third finger, hypothenar eminence and fifth finger. Some papules had a central depression (Figures 1 and 2). These lesions, all asymptomatic, occurred when he was a teenager. No similar lesions were found elsewhere, (e.g. soles of the feet). He was unaware of ever having been exposed to arsenic, and as far as he knew none of his relatives had been affected with the same lesions.
A punch biopsy specimen of one of the palmar papules revealed the presence of compact columns of parakeratotic hyperkeratosis - cornoid lamella - sharply demarcated by a surrounding prominent orthokeratotic hyperkeratosis (Figure 3A). Below the cornoid lamella, the granular layer was thinner, and dyskeratotic cells and vacuolation of some keratinocytes were present (Figure 3B). The underlying papillary dermis presented an inflammatory infiltrate of mononuclear cells. Given the typical clinical manifestations and histopathological findings, the diagnosis of punctate porokeratosis was established. The patient had no complaints or signs of discomfort - the reason why no treatment regime had been hitherto established.
Biopsy of a keratotic palmar papule. (A) Base of epidermal depression with loss of stratum granulosum and presence of compact hyperkeratosis and parakeratosis. (B) Dyskeratosis and vacuolar keratinocytes below the cornoid lamella can be seen.
DISCUSSION
The five major clinical variants of porokeratosis are porokeratosis of Mibelli, disseminated superficial actinic porokeratosis, linear porokeratosis, punctate porokeratosis (PP) and porokeratosis palmaris et plantaris disseminata. PP is a rare variant of porokeratosis which sometimes has a linear configuration. It may be associated with linear or Mibelli porokeratosis.66. Rahbari H, Cordero AA, Mehregan AH. Punctate porokeratosis. A clinical variant of porokeratosis of Mibelli. J Cutan Pathol. 1977;4:338-41. The elementary lesion consists of several punctuate hyperkeratotic seed-like lesions, commonly surrounded by a raised margin located along the palmoplantar surfaces.
As with other variants of porokeratosis, clonal hyperproliferation of atypical keratinocytes leads to the formation of the cornoid lamella, the histopathologic hallmark of porokeratosis. It is a well-demarcated column of compact parakeratosis that frequently depresses the epithelial area with a thin or absent granular layer and occasional vacuolated or dyskeratotic cells. A lymphohistiocytic infiltrate is often described in the underlying dermis. A cornoid lamella is sometimes observed when associated to a variety of inflammatory, hyperplastic and neoplastic dermatoses, thus not specific for porokeratosis.77. Valverde R, Sánchez-Caminero MP, Calzado L, Ortiz de Frutos FJ, Rodríguez-Peralto JL, Vanaclocha F. Dermatomyositis and punctate porokeratotic keratoderma as paraneoplastic syndrome of ovarian carcinoma. Actas Dermosifiliogr. 2007;98:358-60.
The differential diagnosis of PP includes punctate palmoplantar keratoderma, warts, arsenical keratoses, pitted keratolysis, Darier's disease, nevoid basal cell carcinoma syndrome, Cowden's disease and naevus comedonicus (Table 1).22. Herman PS. Punctate porokeratotic keratoderma. Dermatologica. 1973;147:206-13. , 44. Himmelstein R, Lynfield YL. Punctate porokeratosis. Arch Dermatol. 1984; 120:263-4. Punctate porokeratotic keratoderma and spiny keratoderma are also worth considering. It is also worth keeping in mind porokeratotic eccrine ostial and dermal duct nevus (PEODDN), a rare congenital hamartoma of eccrine origin, which may be clinically indistinguishable from PP, although on histological examination it shows multiple cornoid lamella-like parakeratotic columns, associated exclusively with the eccrine duct and ostia.88. Pathak D, Kubba R, Kubba A. Porokeratotic eccrine ostial and dermal duct nevus. Indian J Dermatol Venereol Leprol. 2011;77:174-6. PEODDN is considered by some as a rare variant of porokeratosis.
Punctate palmoplantar keratoderma (Buschke-Fischer-Brauer disease) is an autosomal dominant disease with variable penetrance. Multiple punctate keratoses exist, measuring from 2 to 8 mm in diameter over the entire palmoplantar surfaces. Occasionally a central keratotic core exists which, when removed, leaves a central depression. Although clinically similar to PP, these are histologically distinguished by the presence of a compact column of massive orthohyperkeratosis covering a sharply delimited area of the epidermis rather than a cornoid lamella. Increased thickness of the granular cell layer can also be observed, but no inflammation in the dermis.
Multiple punctate palmoplantar keratoses can also be seen in patients with Darier disease and Cowden disease. A search for other mucocutaneous signs of these disorders should be performed whenever any suspicion of PP arises. The palmoplantar pits of nevoid basal cell carcinoma syndrome and plantar pitted keratolysis are characterized by foci of absent or reduced stratum corneum, given that they are usually not confused with PP. Arsenical keratoses tend to appear later in life and have histological findings similar to those of actinic keratosis.
Punctate porokeratotic keratoderma (PPK) resembles PP, either clinically or histologically It also reveals the presence of parakeratotic cornoid lamellae arising from a decreased or absent granular layer. However, the absence of vacuolar change and dyskeratosis beneath the parakeratotic column, the absence of centrifugally expanding rings of hyperkeratosis, together with the lack of tendency to form plaques, are features that help to differentiate PPK from true porokeratosis.22. Herman PS. Punctate porokeratotic keratoderma. Dermatologica. 1973;147:206-13. Possible associations between PPK and internal malignancy have been reported from time to time. Some authors suggest screening for underlying malignancies in cases of a PPK diagnosis.22. Herman PS. Punctate porokeratotic keratoderma. Dermatologica. 1973;147:206-13. , 77. Valverde R, Sánchez-Caminero MP, Calzado L, Ortiz de Frutos FJ, Rodríguez-Peralto JL, Vanaclocha F. Dermatomyositis and punctate porokeratotic keratoderma as paraneoplastic syndrome of ovarian carcinoma. Actas Dermosifiliogr. 2007;98:358-60. Further studies are needed to determine whether this finding is a real association or a casual occurrence.
Spiny keratoderma (music box spine dermatosis), a dermatosis that has been used interchangeably with PPK, is characterized by multiple tiny keratotic plugs, mimicking the spines on a music box and involving the entire palmoplantar surfaces. In histological terms it shows as columnar parakeratosis, which resembles the cornoid lamella of porokeratosis, overlying a hypogranular epidermis. In 1999, Hashimoto et al suggested that spiny keratoderma is a disease of ectopic hair formation of palms and soles given that the keratotic column is stained with the AE13 (a hair type of keratin).99. Hashimoto K, Toi Y, Horton S, Sun TT. Spiny keratoderma - a demonstration of hair keratin and hair type keratinization. J Cutan Pathol. 1999;26:25-30. Moreover, although some reports point to a link with cancer this has not been conclusively established.1010. Torres G, Behshad R, Han A, Castrovinci AJ, Gilliam AC. "I forgot to shave my hands": a case of spiny keratoderma. J Am Acad Dermatol. 2008;58:344-8. While some lesions of the palms and soles may be spiny in PP, underlying keratinocyte changes (vacuolation and dyskeratosis) target a correct diagnosis.
Accurate treatment for PP has not yet been established, and research continues. Managing PP involves topical treatment such as urea, salicylic acid, and retinoids.44. Himmelstein R, Lynfield YL. Punctate porokeratosis. Arch Dermatol. 1984; 120:263-4. , 66. Rahbari H, Cordero AA, Mehregan AH. Punctate porokeratosis. A clinical variant of porokeratosis of Mibelli. J Cutan Pathol. 1977;4:338-41. Beyond the aesthetic aspect there are no other concerns associated with PP, namely an increased risk of cutaneous cancer.
REFERENCES
-
1Brown FC. Punctate keratoderma. Arch Dermatol. 197;104:682-3.
-
2Herman PS. Punctate porokeratotic keratoderma. Dermatologica. 1973;147:206-13.
-
3Osman Y, Daly TJ, Don PC. Spiny keratoderma of the palms and soles. J Am Acad Dermatol. 1992;26:879-81.
-
4Himmelstein R, Lynfield YL. Punctate porokeratosis. Arch Dermatol. 1984; 120:263-4.
-
5Caccetta TP, Dessauvagie B, McCallum D, Kumarasinghe SP. Multiple minute digitate hyperkeratosis: A proposed algorithm for the digitate keratoses. J Am Acad Dermatol. 2012;67:e49-55.
-
6Rahbari H, Cordero AA, Mehregan AH. Punctate porokeratosis. A clinical variant of porokeratosis of Mibelli. J Cutan Pathol. 1977;4:338-41.
-
7Valverde R, Sánchez-Caminero MP, Calzado L, Ortiz de Frutos FJ, Rodríguez-Peralto JL, Vanaclocha F. Dermatomyositis and punctate porokeratotic keratoderma as paraneoplastic syndrome of ovarian carcinoma. Actas Dermosifiliogr. 2007;98:358-60.
-
8Pathak D, Kubba R, Kubba A. Porokeratotic eccrine ostial and dermal duct nevus. Indian J Dermatol Venereol Leprol. 2011;77:174-6.
-
9Hashimoto K, Toi Y, Horton S, Sun TT. Spiny keratoderma - a demonstration of hair keratin and hair type keratinization. J Cutan Pathol. 1999;26:25-30.
-
10Torres G, Behshad R, Han A, Castrovinci AJ, Gilliam AC. "I forgot to shave my hands": a case of spiny keratoderma. J Am Acad Dermatol. 2008;58:344-8.
-
*
Study conducted at the University of Coimbra Hospitals - Coimbra, Portugal
Publication Dates
-
Publication in this collection
June 2013
History
-
Received
11 Apr 2012 -
Accepted
31 May 2012