Abstracts
This is a qualitative study that aimed to describe the care network of children with special health care needs in different levels of the health care system, during the follow-up after discharge. The data were produced through the development of the dynamics of creativity and sensitivity, the speaking map and the creative and sensitive method, involving five children's families between 2009 and 2011. The caregivers' discourse pointed out that these children's care network comprises the institutional and familial dimensions. The first showed to be broad and diverse but scattered, comprising various health and education professionals. The second consists of members of the close female relatives, such as mothers and grandmothers, showing an exclusively familial care. The expansion and consolidation of multiprofessional care networks is recommended to facilitate the access to health care and quality of life for these children and their family caregivers.
Child health; Pediatric nursing; Family; Caregivers
Estudio cualitativo que objetivó describir la red de cuidados de niños con necesidades especiales en salud en los diferentes niveles de atención después del alta hospitalaria. Los datos fueron producidos con la aplicación de la dinámica de creatividad y sensibilidad, el mapa hablante y del método creativo sensible, con cinco familias de estos niños entre 2009 y 2011. Los discursos de la familia señalaron que la red de cuidados se compone de las dimensiones institucional y familiar. La primera se mostró amplia y diversa, aunque dispersa, compuesto por profesionales de salud y educación. Y en la segunda, la asistencia es exclusivamente familiar, con miembros, todas mujeres, como madres y abuelas. Se recomienda la ampliación y consolidación de la red de cuidado con abordaje multidisciplinar, facilitando el acceso a la atención de salud y la calidad de vida estos niños y sus familiares cuidadores.
Salud del niño; Enfermería pediátrica; Família; Cuidadores
Pesquisa qualitativa que objetivou descrever a rede de cuidados de crianças com necessidades especiais de saúde, acompanhadas em diferentes níveis de atenção, após a alta hospitalar. Os dados foram produzidos por meio da realização da dinâmica de criatividade e sensibilidade, de Mapa Falante e do Método Criativo Sensível, com cinco famílias de crianças, entre 2009 e 2011. Os discursos dos familiares apontaram que a rede de cuidados dessas crianças é constituída pelas dimensões institucional e familial. A primeira mostrou-se ampla e diversificada, porém dispersa, sendo constituída por diversos profissionais da área da saúde e educação. A segunda é composta por integrantes do núcleo familiar feminino, como mães e avós, e apresenta um cuidado exclusivamente familial. Recomenda-se a ampliação e a consolidação de redes de cuidado de natureza multiprofissional para facilitar o acesso à assistência em saúde e a qualidade de vida dessas crianças e suas famílias.
Saúde da criança; Enfermagem pediátrica; Família; Cuidadores
INTRODUCTION
Children with special health care needs (CSHCN) suffer from or are at greater risk of presenting a chronic physical, developmental, behavioral or emotional condition. This condition demands differentiated care and more consultations than other children generally need.11 Rezende JM, Cabral IE. As condições de vida das crianças com necessidades especiais de saúde: determinantes da vulnerabilidade social na rede de cuidados em saúde as Crianças com Necessidades Especiais de Saúde. Rev Pesq Cuid Fundam [online]. 2010 Out-Dez [acesso 2012 Abr 10]; 2(Supl):22-5 Disponível em: http://www.seer.unirio.br/index.php/cuidadofundamental/article/view/773/pdf_68 .
http://www.seer.unirio.br/index.php/cuid...
The CSHCN present continuing care demands that can be temporary or continuing, and require specialized, individual and personalized technical care. These children's hospitalization are frequent and sometimes long, causing greater diagnostic complexity.22 Góes FGB, Cabral IE. Crianças com necessidades especiais de saúde e suas demandas de cuidado. Rev Pesq Cuid Fundam [online]. 2010 Abr-Jun [acesso 2012 Mai 20]; 2(2):889-901 Disponível em: http://www.sumarios.org/sites/default/files/pdfs/64821_7337.PDF .
http://www.sumarios.org/sites/default/fi...
In general, these children are survivors of the technological advances in the health area, which have changed the epidemiological profile of childhood. These changes have led to the decline in the childhood mortality rates registered in recent decades, as opposed to the increase number of chronic illnesses in childhood.
Like in other countries, the children's survival profile has changed. A study of children who graduate from a Neonatal Intensive Care Unit found that 16% of them have special health needs.33 Arrué AM, Neves ET, Mathias CV, Jantsch LB, Pieszack GM, Naidon AN. Niños con necesidades especiales de salud egresados de cuidados intensivos neonatal. Evidentia [online]. 2014 [acesso 2014 Fev 25]; 11(45): Disponível em: http://www.index-f.com/evidentia/n45/ev8091.php .
http://www.index-f.com/evidentia/n45/ev8...
Nevertheless, research is needed on the nature of their health demands, survival conditions and the care network of this new child group.
The CSHCN' special needs include complex health needs, which their caregivers need to perform in the home context.44 Neves ET, Cabral IE. Empoderamento da mulher cuidadora de crianças com necessidades especiais de saúde. Texto Contexto Enferm. 2008 Jul-Set; 17(3):552-60. The families face constant quests in search of specialized care and demand a multiprofessional care network that is capable of contributing to their empowerment process.
In that context, the family creates its own networks in search of this specialized care, with a view to guaranteeing appropriate care to the CSHCN. Thus, the care networks are constituted in care actions in the health and disease process. These networks are individualized and are defined by their size, density and composition, permitting the development of different functions, ranging from social campaigns to emotional support, promoting the support needed to serve as a cognitive guide and counsel. This care network can also contribute with material resources and services, offering material goods and access to new contacts, besides including the people in other social networks as a form of sharing experiences.55 Gutierrez DMD, Minayo MCS. Família, redes sociais e saúde: o imbricamento necessário. In: Seminário Internacional Fazendo Gênero, 8, Florianópolis, 2008. Anais... Florianópolis: UFSC, 2008. p. 4.Disponível em: http://universaleducacaoecultura.webs.com/documents/Fam%C3%83%C2%ADlia,%20redes%20sociais%20e%20sa%C3%83%C2%BAde.pdf
http://universaleducacaoecultura.webs.co...
In view of the problematic dispersion of the CSHCN' care networks after the hospital discharge, the networks that support the CSHCN and their relatives need to be strengthened, both the institutional networks and the social networks. Hence, the articulation between the health services and the networks that establish bonds with the CSHCN is fundamental for the visibility of this group and its health demands.
Based on this problem, it was questioned how the care network of children with special health needs is constituted after the hospital discharge. In view of the above, this research aimed to describe the care network of children with special health needs at different care levels after the hospital discharge.
METHOD
A qualitative research with a participatory approach was undertaken as part of a larger research entitled "Children discharged from neonatal intensive care: characterization of special health needs and access to health monitoring services in Santa Maria, RS - CSHCN Research".
This paper refers to the second phase, when the qualitative data of the above mentioned research were produced. The subjects were the family caregivers of the children discharged from the Neonatal Intensive Care Unit (NICU), coming from the city of Santa Maria-RS and registered in the database of the research "CSHCN" (2002-2006).
The data were collected between 2009 and 2011. The participants were 11 subjects from five families of the CSHCN drawn. As the database included children born between 2002 and 2006, one CSHCN was drawn for each year and the families were contacted.
The qualitative data were developed based on the Creative and Sensitive Method (CSM),66 Cabral IE. Aliança de saberes no cuidado e estimulação da criança-bebê: concepções de estudantes e mães no espaço acadêmico de enfermagem. Rio de Janeiro (RJ): Editora da Escola de Enfermagem Anna Nery; 1999. including five Creativity and Sensitivity Dynamics (CSD) - Speaker Map,44 Neves ET, Cabral IE. Empoderamento da mulher cuidadora de crianças com necessidades especiais de saúde. Texto Contexto Enferm. 2008 Jul-Set; 17(3):552-60. during home visits, which took place after preliminary telephone contact with each of the families of the CSHCN drawn. The CSM combines consolidated qualitative research techniques, such as collective interview, participant observation and group discussion, associated with the CSDs. These phases are developed during the group meeting, when the discussion question guides the collective interview. The observation (body language, gestures, etc.) is done during the meeting and is registered by the research aid(s) in a field diary. The group discussion takes place during the CSD. The subjects express themselves through the artistic production (design of monitoring networks of the CSHCN after the discharge), in response to the discussion question that was presented to the group, permitting the creation of a dialogic, dialectic and plural space between the subjects and the researcher.66 Cabral IE. Aliança de saberes no cuidado e estimulação da criança-bebê: concepções de estudantes e mães no espaço acadêmico de enfermagem. Rio de Janeiro (RJ): Editora da Escola de Enfermagem Anna Nery; 1999.
To develop the CSDs, the following guiding questions were used: starting from your house, what health services do you take [name of CSHCN] to? Who are the people or institutions that help? Where do you go with the CSHCN?
To characterize the subjects involved in the study, an interview was held before the meeting with the family caregivers of the CSHCN. The meeting was audio-recorded and, afterwards, the statements were fully transcribed.
The qualitative data, obtained through the audio-recordings of the interviews and group discussions, were transcribed and analyzed through French discourse analysis (DA),77 Orlandi EP. Análise de discurso: princípios e procedimentos. 10ª ed. Campinas (SP): Pontes; 2012. which does not only aim to know the language, but to understand it as symbolic work and part of the general work, forming man and history. Thus, one can know what makes man into a special being, able to attribute and receive meaning.7
The discourse analysis took place at three times. First, the subjects' discourse was transcribed, adding movement through the use of orthographical resources, representing the phase of linguistic materiality. Next, the borderline situations were selected, extracted from the full text of the transcribed dynamics, and included in the analyses to compose the research corpus, characterizing the organization phase of the data for analysis. In the third phase - analysis and interpretation - the analytic tools typical of DA were used, such as metaphor, polysemy and paraphrase, so as to extract the meaning of the text. The following orthographical resources were used to grant linguistic materiality to the text, representing the discourse movement: /: short reflexive pause; //: long reflexive pause; ///: very long reflexive pause; ...: incomplete statement; #: interruption of a person's enunciation; [ ] - completing the verbal thought enounced in the same statement; '...': single inverted commas, which indicate the statement or text of someone cited inside another person's enunciation; and (...) which indicates a cut in the subjects' discourse.
The research was conduced according to the ethical and legal precepts of Resolution 196/96 and the subjects signed the Free and Informed Consent Form. It is highlighted that the subjects received fictitious names, guaranteeing their anonymity. The project received approval from the Ethics Committee under number 0003.0.243.000-08.
RESULTS
Initially, in Figure 1, the CSHCN are characterized, as well as their special health care needs (SHCN), care demands and the family caregivers.
The spoken and imaging discourse of the CSHCN's family caregivers permitted knowing these families' trajectory in search of qualified care for their children.
Next, two caregivers' enunciation is presented, who described their artistic production (AP):
(...) here [points at the drawing] I am leaving my home (...) and I took Guilherme to the service [Primary Health Care Unit] (...) Because he convulsed... (...) When the convulsions happen, the first aid he gets at the health service (...) then they send him to the hospital (...)There's the federal university, the [name of the university] there where we took him to treat with the neurologist and gastro [gastroenterologist] and [where he] gets physiotherapy once a week (...) (Vera).
[...] it's, like, I think / the EC [emergency care], the [name of the hospital], they're his health references. Ah!! There's one here at the school too (...). He is monitored by the neuro [neurologist] (...) and he's from the SAF [Speech, language and hearing care service], the otorhino [otorhinolaryngologist] (...). And the doctors and the pediatricians, everything at the UH[University Hospital] (...) (Ana).
Figure 1 below illustrates a hardly articulated care network, in which the family represented only the institutional health services the child attends.
The CSHCN's caregivers need to attend different health care services, such as the primary health care unit, the emergency care services and the university as a reference for outpatient care and monitoring in different medical specialties. In addition, the physiotherapists and speech, language and hearing therapists are part of the CSHCN's institutional health care network.
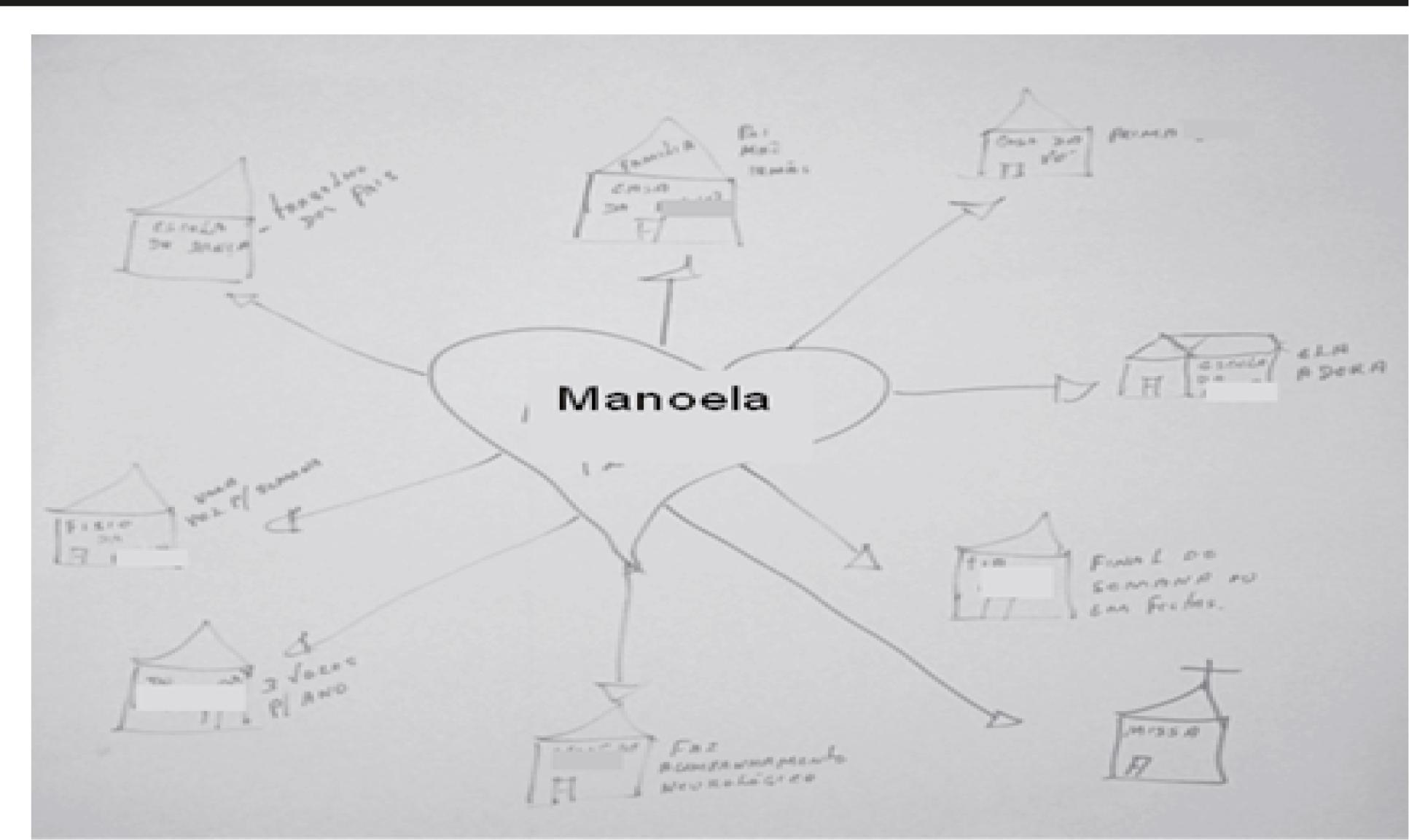
In the AP of Manoela's relatives, figure 2, besides an institutional network, a broad but geographically dispersed familial network can also be observed.
The geographical dispersion and the different services the child uses are presented in figure 2 and in the following enunciations:
no, [the physiotherapy] is at APAE. (...) The school! [points at the drawing] Which she loves! (Marina). And to André: it's the doctor [name of the pediatrician]. (...) it's not that frequent [that the CSHCN attends]. At the physiotherapy we received a lot of orientation, during the initial treatments (...) (André).
The family members mention different health services and professionals, among which the following stand out: medical team; speech, language and hearing therapists; physiotherapists; occupational therapists; dentist; pedagogue; besides the teachers of the CSHCN who attend school.
(...) the [Occupational therapist] comes once a week. (...) On Tuesday, Isabela goes there to the...// [name of the CSHCN's school] (...) She goes to the dentist's / every Wednesday.(...) And here on Wednesday as well soon afterwards there's the ACDV, // which is the Association of the Visually Impaired with the [name of the pedagogue] (...) And there's more, on Fridays there's occupational therapy again at the [name of the university]. /// (...) (Luisa).
When asked about how they conciliate the employment and the care for the CSHCN, the caregivers show to give up their job to exclusively dedicate themselves to the care for the child:
I quit [working] (...) because after I assumed the responsibility for him, then I started taking him more to the speech [speech, language and hearing therapist], he used to go there once a week before I started to take care of him. And then she [daughter-in-law] said she wanted to work, that she was going to work, so I said: 'I quit my job and take care of him and you go to work because I can [resource - husband's retirement benefit] (...), so I can survive (...)'(Ana).
According to Ana, João's grandmother, she had to give up her job to fully take care of the child, thus allowing the parents to work in order to guarantee the resources to pay for the costs of the CSHCN's care demands.
When discussing the CSHCN's use of the primary care services, the relatives enounced: there is, there is. But we... # (...) live close to the EC [Municipal Emergency Care] and we go there all the time. (...) (André). And what the access to the primary care services is concerned: because what happens at these Primary Care Services is that you have to go there in advance, take a ticket early, sometime you go there and do not get it [care]. So we end up giving up (Marina).
The primary care services appeared in the family members' discourse as a reference because of there geographical proximity to the home, despite the difficult access to get care and solve the CSHCN's problems:
[...] not Patricia. Only when it's a simple flu, something trivial. Because it's difficult for us to get a ticket there, because you either have to get up very early, you have to go there at three, four o'clock in the morning to be able to get something, so she, Patricia, we take here and go straight to the UH [University Hospital], right? (Julia).
In addition, the frailty of the child's clinical condition makes the family caregivers turn to emergency care services due to the need for immediate care. And, in general, the problems with the child happen beyond the primary health care services' functioning hours.
As regards the care network units responsible for the CSHCN's leisure and culture, the family members mentioned:
It's on the square [laughs]. At church it's on Wednesdays and Sundays (Julia); And: Yes! Because we, like: during the holidays she comes here [referring to the dance school] with us every day (...).We forgot to tell that she goes to mass!! I'll put the church here! (...) she goes to mass and it's in front...# (André).
In the child's institutional network, the family members described leisure and culture tools, like the recreation square and the church. For one of the CSHCN's, a dance school was included, where her parents work, where the child had contact with other people, besides being stimulated by the dance activities.
The following social reference points emerged in the care network, which support the family caregivers: we are ourselves here. (...) It's (...). My son. His grandmother lives next door, right? [laughs]. (...) then there's her aunt, because she goes to her uncles too (Julia).
As perceived, the care is exclusively familial; many CSHCN have only one main caregiver or who divides the care with some close relatives, who are generally female and come from the nuclear family, including sisters, uncles, grandmothers and godmothers: Isabela, her grandmother and her great-grandmother, .../ we here. (...) my daughter, the boys [uncles]. Because my brother is there and he's singing a song to her and she sings, my son too, my husband goes also, tells a story, everyone [the nuclear family]participates (Luisa).
Thus, it was verified that the CSHCN's care network consists of the institutional and family dimensions. The first was broad and diversified but dispersed, consisting of different health and education professionals. The second includes members of the nuclear family and the care is exclusively familial. The leisure and socialization network is restricted to the recreation square, and the mass is a reference for spirituality.
DISCUSSION
The institutional dimension of the care network of children with special health care needs
The study indicates the nature of the bonds as a determining factor in the functionality of the network, meaning that, the stronger the bonds, the stronger the network will be.88 Leal JR, Cabral IE, Perreault M. Experiência Brasil-Canadá no cuidado social e na saúde da criança com necessidades especiais: aproximações e distanciamentos. Interfaces Brasil/Canadá. 2010; (11):95-119. Another relevant factor in the intensification process of the bonds is the contact with the services and people engaged in care for the child. A care network is revealed that rests on the family and on the tertiary health services.99 Neves ET, Andres B, Silveira A, Arrué AM. A rede social de cuidados de uma criança com necessidade especial de saúde. Rev Eletr Enf [online]. 2013 Abr-Jun [acesso 2013 Mai 21]; 15(2):533-40 Disponível em: http://dx.doi.org/10.5216/ree.v15i2.17064. .
http://dx.doi.org/10.5216/ree.v15i2.1706...
The relation between people's health and the establishment of a stable and active social network is considerable, as the network influences people's health and is influenced by their health condition.1010 Andreani G, Custódio ZAO, Crepaldi MA. Tecendo as redes de apoio na prematuridade. Rev Aletheia. 2006; (24):115-26.
Although the legislation of the Unified Health System (SUS) guarantees the equalitarian right and access to health, the CSHCN's relatives are often confronted with difficulties to get access to the health services and with errors in the referral and counter-referral system. The access to the health services shows to be selective and focused on specialized services, evidencing a contradiction between the law and the social legitimacy of the right to health.1111 Klassmann J, Kochia KRA, Furukawa TS, Higarashi IH, Marcon SS. Experiência de mães de crianças com leucemia: sentimentos acerca do cuidado domiciliar. Rev Esc Enferm USP. 2008; 42(2):321-30. This infringes on the SUS principles of integrality and universal access.1212 Neves ET, Silveira A. Desafios para os cuidadores familiares de crianças com necessidades especiais de saúde: contribuições da enfermagem. Rev Enferm UFPE [online] 2013 Mai [acesso 2013 Jun 12]; 7(5):1458-62 Disponível em: http://www.revista.ufpe.br/revistaenfermagem/index.php/revista/article/viewArticle/3229 .
http://www.revista.ufpe.br/revistaenferm...
The CSHCN's health needs are complex and demand care from different professionals, located in distinct places, which requires exclusive and exhaustive dedication to care from the caregiver. The caregivers needs to manage a diversified routine of care and consultations, which is complex and located in geographically distinct places.1313 Neves ET, Cabral IE, Silveira A. Rede familial de crianças com necessidades especiais de saúde: implicações para a enfermagem. Rev Latino-Am Enfermagem [online]. 2013 Mar-Abr [acesso 2013 Jun 12]; 21(2):[09 telas] Disponível em: http://www.scielo.br/pdf/rlae/v21n2/pt_0104-1169-rlae-21-02-0562.pdf .
http://www.scielo.br/pdf/rlae/v21n2/pt_0...
As regards the health services in the CSHCN's institutional network, preferential access is observed for those places that deliver tertiary care, to the detriment of primary care services. This demonstrates the difficulties to get access to the health services for the sake of the continuity of the health treatment after the child's discharge from hospital.
In a study undertaken in Santa Maria-RS in 2009, it was identified that the CSHCN's relatives seek hospital care when they do not find spaces in the coomunity.99 Neves ET, Andres B, Silveira A, Arrué AM. A rede social de cuidados de uma criança com necessidade especial de saúde. Rev Eletr Enf [online]. 2013 Abr-Jun [acesso 2013 Mai 21]; 15(2):533-40 Disponível em: http://dx.doi.org/10.5216/ree.v15i2.17064. .
http://dx.doi.org/10.5216/ree.v15i2.1706...
The same result was identified in a research developed in 2011, in which relatives of CSHCN referred to the primary care services' lack of preparation to receive these children, making the family members seek tertiary services.1414 Zamberlan KC, Neves ET, Silveira A. institutional care network of children with special health care needs. J Nurs UFPE. 2012 Mai; 6(5):1015-23.
The family members consider the access conditions to the primary care services difficulty and the number of patients attended per shift is limited. In another study on the theme,1515 Souza ECF, Vilar RLA, Rocha NSPD, Uchoa AC, Rocha PM. Acesso e acolhimento na atenção básica: uma análise da percepção dos usuários e pro?ssionais de saúde. Cad Saúde Pública. 2008; 24(Sup1):100-10. the patients mentioned the insufficient number of professionals to attend to the demand of users who depend on the service, associated with the lack of work organization.
In the United States of America (USA), this reality is also experienced, as 48.8% of CSHCN's relatives mentioned difficulties to get access to medical services and 31% to other services.1616 Kuo DZ, Cohen E, Agrawal R, Berry JG, Casey PH. A national profile of caregiver challenges among more medically complex children with special health care needs. Arch Pediatr Adolesc Med. 2011 Nov; 165(11):1020-6. Differently from the Brazilian reality however, in the USA, there is no public and universal health service.
For the CSHCN, the caregivers choose emergency care for situations that could be solved at primary care services. The users turn to other services, such as emergency care, to treat acute cases as if it were emergencies. This fact happens because the families expect the immediate solution of the case, despite the long waiting times at emergency services.1515 Souza ECF, Vilar RLA, Rocha NSPD, Uchoa AC, Rocha PM. Acesso e acolhimento na atenção básica: uma análise da percepção dos usuários e pro?ssionais de saúde. Cad Saúde Pública. 2008; 24(Sup1):100-10.
The CSHCN's institutional network also includes people who offer support in daily life, such as some multiprofessional team professionals in the complex care network these children require. A study involving chronic patients indicates that they mention people, beyond the family group, who offer support to the caregivers, establishing interdependent and affective relationships.1717 Silveira CL, Budó MLD, Silva FM, Beuter M, Schimith, MD. Rede social das cuidadoras de familiares com doença crônica incapacitante no domicílio: implicações para a enfermagem. Ciênc Cuid Saúde. 2009 Out-Dez; 8(4):667-74. In general, the caregiver attends to the child's needs, reducing his/her relationship networks to the closest relatives and turning to spirituality, represented by visits to mass in this study, making the support network fragile and restricted.1313 Neves ET, Cabral IE, Silveira A. Rede familial de crianças com necessidades especiais de saúde: implicações para a enfermagem. Rev Latino-Am Enfermagem [online]. 2013 Mar-Abr [acesso 2013 Jun 12]; 21(2):[09 telas] Disponível em: http://www.scielo.br/pdf/rlae/v21n2/pt_0104-1169-rlae-21-02-0562.pdf .
http://www.scielo.br/pdf/rlae/v21n2/pt_0...
The presence of the child in church, where the family receives comfort, revealed the theme spiritual support. The sensation of feeling spiritually welcomed makes the family get closer to religious rituals, which grant them hope and comfort, besides internal peace, which often is not achieved in any other way.1818 Hayakawa LY, Marcon SS, Higarashi IH, Waidman MAP. Rede social de apoio à família de crianças internadas em uma unidade de terapia intensiva pediátrica. Rev Bras Enferm. 2010 Mai-Jun; 63(3):440-5. For the people who go through disease situations, religion ends up playing the role of emotional support, strengthening the hope, renewing the strengths, helping them to live and cope with the difficulties.1717 Silveira CL, Budó MLD, Silva FM, Beuter M, Schimith, MD. Rede social das cuidadoras de familiares com doença crônica incapacitante no domicílio: implicações para a enfermagem. Ciênc Cuid Saúde. 2009 Out-Dez; 8(4):667-74.
The familial dimension of the care network of children with special health needs
The study revealed that the family members need to deliver complex care to these children at home, even without background knowledge and without the technology available in the hospital context. The care demands of the CSHCN include the routine performance of complex continuing care, such as relief probe measures, aspiration, tube feeding or gastrostomy, bed bathing, drain care and dressings. After the child's discharge, the family caregiver starts to perform various procedures at home, which requires skill, management and adaptation of the home environment for the sake of care.44 Neves ET, Cabral IE. Empoderamento da mulher cuidadora de crianças com necessidades especiais de saúde. Texto Contexto Enferm. 2008 Jul-Set; 17(3):552-60.
In view of the CSHCN's diagnosis, in general, the subjects' way of being and positioning in the family group are redimensioned.1919 Motta MGC, Issi HB, Milbrath VM, Ribeiro NRR, Resta DG. Famílias de crianças e adolescentes no mundo do hospital: ações de cuidado. In: Elsen I, Souza AIJ, Marcon SS. Enfermagem à família: dimensões e perspectivas. Maringá (PR): Eduem; 2011. p.73-85. The family of a child with special health care needs goes through a readaptation in its way of life and starts to dedicate itself to exclusive care for the CSHCN.
When a child gets ill, the entire family engages in the process. It does not matter whether the disease is acute or chronic, nor the care required, as the child and family are influenced. The family starts to live with the child's disease and to link his/her survival to the familial care.2020 Rossi CS, Rodrigues BMRD. Típico da ação do profissional de enfermagem quanto ao cuidado familial da criança hospitalizada. Acta Paul Enferm. 2010 Out; 23(5):640-5. In most cases, the care activities the family performs are executed in a solitary and uninterrupted manner.2121 Brondani CM, Beuter M, Alvim NAT, Szareski C, Rocha LS. Cuidadores e estratégias no cuidado ao doente na internação domiciliar. Texto Contexto Enferm. 2010 Jul-Set; 19(3):504-10. This can be observed in the enunciations of the family members who mentioned they gave up working and having a social life to exclusively dedicate themselves to care for the child, exposing them to the development of physical and mental health problems.2222 Earle A, Heymann J. Protecting the health of employees caring for family members with special health care needs. Soc Sci Med. 2011 Jul; 73(1):68-78.
The familial care network is reduced to the main female family caregivers from the nuclear family (mother, grandmother and godmother). The familial care takes the form of actions and interactions present in the life of each family group, aiming for wellbeing, personal accomplishment and development, through interactions among the members of this family, according to the understanding of the existential situation.2323 Elsen I, Penna CMM, Althoff CR, Bub LIR, Patrício ZM. Marcos para prática de enfermagem com famílias. Florianópolis (SC): Ed. UFSC; 1994. Hence, the familial care ends up being executed according to the background knowledge or the knowledge gained in the course of the family's practice.
The family caregivers described the limitations experienced in care for the CSHCN, aggravated by the restricted social network and the child's vulnerability. Although the family caregiver is the main responsible for care for the CSHCN, the family needs to find support in the support networks after the hospital discharge. Hence, the health professionals need to pay attention to the center of the care, where the children and their families are, as beings in vulnerable conditions. 2424 Cabral IE. Desafios e perspectivas do cuidar de enfermagem na saúde da criança. Esc Anna Nery Rev Enferm. 2009 Out-Dez;13(4):691-3.
CONCLUSION
For the five families who took part in this study, the care network showed multiple facets, including the institutional and familial dimensions. The institutional area was broad and diversified, including different health and education professionals. The primary care services were appointed as difficult to access and difficulties were mentioned in the referral and counter-referral services. The emergency care services are prioritized because of their agility and problem-solving ability, independently of the functioning hours.
The familial network showed to be based on solitary and often female care. The family dynamics are modified and gain new configurations to respond to the CSHCN's care demands. As a strategy, the family caregivers create social support connections in the institutional network, with the community, the education, leisure and spiritual support network, in search of appropriate treatment.
The caregivers weave these care networks, depending on the personal and family knowledge and how easily they can access the services, often with the help of third parties, which infringes on the principles of the Brazilian public health system SUS. Patients without these facilities are abandoned to their fate, fighting for their rights in a solitary manner.
Moreover, due to the clinical fragility and the complexity of the diagnosis, the CSHCN need a multiprofessional care network to monitor their health after the discharge. Therefore, the health professionals need to know the daily life of the CSHCN and their family members, paying attention to the need for monitoring in the primary care network, so as to minimize renewed hospitalizations. Therefore, starting from the discharge, they need help, through multiprofessional care networks that grant a better life, not only for the CSHCN, but also for their family caregivers, acting as facilitators of these families' empowerment.
One study limitation is the difficulty to locate the subjects, due to the incomplete data in the patient histories. In addition, due to the children's care demand, the family caregivers had to reorganize the entire care routine to attend to the researchers at home.
REFERENCES
-
1Rezende JM, Cabral IE. As condições de vida das crianças com necessidades especiais de saúde: determinantes da vulnerabilidade social na rede de cuidados em saúde as Crianças com Necessidades Especiais de Saúde. Rev Pesq Cuid Fundam [online]. 2010 Out-Dez [acesso 2012 Abr 10]; 2(Supl):22-5 Disponível em: http://www.seer.unirio.br/index.php/cuidadofundamental/article/view/773/pdf_68 .
» http://www.seer.unirio.br/index.php/cuidadofundamental/article/view/773/pdf_68 -
2Góes FGB, Cabral IE. Crianças com necessidades especiais de saúde e suas demandas de cuidado. Rev Pesq Cuid Fundam [online]. 2010 Abr-Jun [acesso 2012 Mai 20]; 2(2):889-901 Disponível em: http://www.sumarios.org/sites/default/files/pdfs/64821_7337.PDF .
» http://www.sumarios.org/sites/default/files/pdfs/64821_7337.PDF -
3Arrué AM, Neves ET, Mathias CV, Jantsch LB, Pieszack GM, Naidon AN. Niños con necesidades especiales de salud egresados de cuidados intensivos neonatal. Evidentia [online]. 2014 [acesso 2014 Fev 25]; 11(45): Disponível em: http://www.index-f.com/evidentia/n45/ev8091.php .
» http://www.index-f.com/evidentia/n45/ev8091.php -
4Neves ET, Cabral IE. Empoderamento da mulher cuidadora de crianças com necessidades especiais de saúde. Texto Contexto Enferm. 2008 Jul-Set; 17(3):552-60.
-
5Gutierrez DMD, Minayo MCS. Família, redes sociais e saúde: o imbricamento necessário. In: Seminário Internacional Fazendo Gênero, 8, Florianópolis, 2008. Anais... Florianópolis: UFSC, 2008. p. 4.Disponível em: http://universaleducacaoecultura.webs.com/documents/Fam%C3%83%C2%ADlia,%20redes%20sociais%20e%20sa%C3%83%C2%BAde.pdf
» http://universaleducacaoecultura.webs.com/documents/Fam%C3%83%C2%ADlia,%20redes%20sociais%20e%20sa%C3%83%C2%BAde.pdf -
6Cabral IE. Aliança de saberes no cuidado e estimulação da criança-bebê: concepções de estudantes e mães no espaço acadêmico de enfermagem. Rio de Janeiro (RJ): Editora da Escola de Enfermagem Anna Nery; 1999.
-
7Orlandi EP. Análise de discurso: princípios e procedimentos. 10ª ed. Campinas (SP): Pontes; 2012.
-
8Leal JR, Cabral IE, Perreault M. Experiência Brasil-Canadá no cuidado social e na saúde da criança com necessidades especiais: aproximações e distanciamentos. Interfaces Brasil/Canadá. 2010; (11):95-119.
-
9Neves ET, Andres B, Silveira A, Arrué AM. A rede social de cuidados de uma criança com necessidade especial de saúde. Rev Eletr Enf [online]. 2013 Abr-Jun [acesso 2013 Mai 21]; 15(2):533-40 Disponível em: http://dx.doi.org/10.5216/ree.v15i2.17064. .
» http://dx.doi.org/10.5216/ree.v15i2.17064 -
10Andreani G, Custódio ZAO, Crepaldi MA. Tecendo as redes de apoio na prematuridade. Rev Aletheia. 2006; (24):115-26.
-
11Klassmann J, Kochia KRA, Furukawa TS, Higarashi IH, Marcon SS. Experiência de mães de crianças com leucemia: sentimentos acerca do cuidado domiciliar. Rev Esc Enferm USP. 2008; 42(2):321-30.
-
12Neves ET, Silveira A. Desafios para os cuidadores familiares de crianças com necessidades especiais de saúde: contribuições da enfermagem. Rev Enferm UFPE [online] 2013 Mai [acesso 2013 Jun 12]; 7(5):1458-62 Disponível em: http://www.revista.ufpe.br/revistaenfermagem/index.php/revista/article/viewArticle/3229 .
» http://www.revista.ufpe.br/revistaenfermagem/index.php/revista/article/viewArticle/3229 -
13Neves ET, Cabral IE, Silveira A. Rede familial de crianças com necessidades especiais de saúde: implicações para a enfermagem. Rev Latino-Am Enfermagem [online]. 2013 Mar-Abr [acesso 2013 Jun 12]; 21(2):[09 telas] Disponível em: http://www.scielo.br/pdf/rlae/v21n2/pt_0104-1169-rlae-21-02-0562.pdf .
» http://www.scielo.br/pdf/rlae/v21n2/pt_0104-1169-rlae-21-02-0562.pdf -
14Zamberlan KC, Neves ET, Silveira A. institutional care network of children with special health care needs. J Nurs UFPE. 2012 Mai; 6(5):1015-23.
-
15Souza ECF, Vilar RLA, Rocha NSPD, Uchoa AC, Rocha PM. Acesso e acolhimento na atenção básica: uma análise da percepção dos usuários e pro?ssionais de saúde. Cad Saúde Pública. 2008; 24(Sup1):100-10.
-
16Kuo DZ, Cohen E, Agrawal R, Berry JG, Casey PH. A national profile of caregiver challenges among more medically complex children with special health care needs. Arch Pediatr Adolesc Med. 2011 Nov; 165(11):1020-6.
-
17Silveira CL, Budó MLD, Silva FM, Beuter M, Schimith, MD. Rede social das cuidadoras de familiares com doença crônica incapacitante no domicílio: implicações para a enfermagem. Ciênc Cuid Saúde. 2009 Out-Dez; 8(4):667-74.
-
18Hayakawa LY, Marcon SS, Higarashi IH, Waidman MAP. Rede social de apoio à família de crianças internadas em uma unidade de terapia intensiva pediátrica. Rev Bras Enferm. 2010 Mai-Jun; 63(3):440-5.
-
19Motta MGC, Issi HB, Milbrath VM, Ribeiro NRR, Resta DG. Famílias de crianças e adolescentes no mundo do hospital: ações de cuidado. In: Elsen I, Souza AIJ, Marcon SS. Enfermagem à família: dimensões e perspectivas. Maringá (PR): Eduem; 2011. p.73-85.
-
20Rossi CS, Rodrigues BMRD. Típico da ação do profissional de enfermagem quanto ao cuidado familial da criança hospitalizada. Acta Paul Enferm. 2010 Out; 23(5):640-5.
-
21Brondani CM, Beuter M, Alvim NAT, Szareski C, Rocha LS. Cuidadores e estratégias no cuidado ao doente na internação domiciliar. Texto Contexto Enferm. 2010 Jul-Set; 19(3):504-10.
-
22Earle A, Heymann J. Protecting the health of employees caring for family members with special health care needs. Soc Sci Med. 2011 Jul; 73(1):68-78.
-
23Elsen I, Penna CMM, Althoff CR, Bub LIR, Patrício ZM. Marcos para prática de enfermagem com famílias. Florianópolis (SC): Ed. UFSC; 1994.
-
24Cabral IE. Desafios e perspectivas do cuidar de enfermagem na saúde da criança. Esc Anna Nery Rev Enferm. 2009 Out-Dez;13(4):691-3.
-
1
Research funded by the Fundação de Amparo à Pesquisa do Estado do Rio Grande do Sul - FAPERGS.
Publication Dates
-
Publication in this collection
Apr-Jun 2015
History
-
Received
22 Oct 2013 -
Accepted
17 Jan 2014