
ABSTRACT
Background:
The treatment of advanced gastric cancer with curative intent is essentially surgical and chemoradiotherapy is indicated as neo or adjuvant to control the disease and prolong survival.
Aim:
To assess the survival of patients undergoing subtotal or total gastrectomy with D2 lymphadenectomy followed by adjuvant chemoradiotherapy.
Methods:
Were retrospectively analyzed 87 gastrectomized patients with advanced gastric adenocarcinoma, considered stages IB to IIIC and submitted to adjuvant chemoradiotherapy (protocol INT 0116). Tumors of the esophagogastric junction, with peritoneal implants, distant metastases, and those that had a compromised surgical margin or early death after surgery were excluded. They were separated according to the extention of the gastrectomy and analyzed for tumor site and histopathology, lymph node invasion, staging, morbidity and survival.
Results:
The total number of patients who successfully completed the adjuvant treatment was 45 (51.7%). Those who started treatment and discontinued due to toxicity, tumor-related worsening, or loss of follow-up were 10 (11.5%) and reported as incomplete adjuvant. The number of patients who refused or did not start adjuvant treatment was 33 (48.3%). Subtotal gastrectomy was indicated in 60 (68.9%) and total in 27 (31.1%) and this had a shorter survival. The mean resected lymph nodes was 30.8. Staging and number of lymph nodes affected were predictors of worse survival and the more advanced the tumor. Patients undergoing adjuvant therapy with complete chemoradiotherapy showed a longer survival when compared to those who did it incompletely or underwent exclusive surgery. On the other hand, comparing the T4b (IIIB + IIIC) staging patients who had complete adjuvance with those who underwent the exclusive operation or who did not complete the adjuvant, there was a significant difference in survival.
Conclusion:
Adjuvant chemoradiotherapy presents survival gain for T4b patients undergoing surgical treatment with curative intent.
HEADINGS:
Gastric neoplasm; Adjuvant therapy; Gastrectomy
RESUMO
Racional:
O tratamento do câncer gástrico avançado com intenção curativa é essencialmente cirúrgico e a quimiorradioterapia está indicada como neo ou adjuvância para controlar a doença e prolongar a sobrevida.
Objetivos:
Avaliar a sobrevida dos doentes submetidos à gastrectomia subtotal ou total com linfadenectomia D2 seguidos de quimiorradioterapia adjuvante.
Métodos:
Foram analisados retrospectivamente 87 gastrectomizados portadores de adenocarcinoma gástrico avançado considerandos estádios IB até IIIC e submetidos à quimiorradioterapia adjuvante (protocolo INT 0116). Foram excluídos os tumores da transição esofagogástrica, com implantes peritoneais, metástases à distância e os que após a operação apresentaram margem cirúrgica comprometida ou óbito precoce. Foram separados quanto à extensão da gastrectomia e analisados em relação ao local e histopatologia do tumor, invasão linfonodal, estadiamento, morbidade e sobrevida.
Resultados:
O número de doentes que conseguiu completar o esquema adjuvante na sua totalidade foi de 45 (51,7%). Os que iniciaram o tratamento e interromperam por toxicidade, piora relacionada ao tumor, ou perda de seguimento foram 10 (11,5%) e relacionados como adjuvância incompleta. O número de doentes que recusou ou não iniciou o tratamento adjuvante foi de 33 (48,3%). A gastrectomia subtotal foi indicada em 60 (68,9%) e a total em 27 (31,1%) e esta apresentou menor sobrevida. A média de linfonodos ressecados foi de 30,8. O estadiamento e o número de linfonodos acometidos foram preditores de pior sobrevida e quanto mais avançado foi o tumor. Os pacientes submetidos à terapia adjuvante com quimiorradioterapia completa mostraram sobrevida maior quando comparados àqueles que a fizeram de forma incompleta ou submetidos à operação exclusiva. Por outro lado, comparando-se os doentes estádios T4b (IIIB + IIIC) que tiveram adjuvância completa com os submetidos à operação exclusiva ou que não completaram a adjuvância, houve significativa diferença na sobrevida.
Conclusão
- A quimiorradioterapia adjuvante apresenta ganho de sobrevida para doentes em estádio T4b submetidos ao tratamento cirúrgico com intenção curativa.
DESCRITORES:
Neoplasias gástricas; Terapias adjuvantes; Gastrectomia
INTRODUCTION
Despite the declining incidence in the rest of the world, gastric cancer appears third in incidence among men and fifth in women in Brazil. Due to the aggressiveness of the disease and the symptoms being nonspecific, most patients already have advanced tumors at the time of diagnosis, providing low survival rates77 Brazil, Ministry of Health National Cancer Institute. [database on the Internet]. In 2018. Available from: https://www.inca.gov.br/tipos-de-cancer/cancer-de-estomago.
https://www.inca.gov.br/tipos-de-cancer/...
,1313 Ferlay J, Soerjomataram I, Dikshit R, Eser S, Mathers C, Rebelo M, Parkin DM, Forman D, Bray F. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015;136: E359-86.- doi: 10.1002/ijc.29210.
https://doi.org/10.1002/ijc.29210...
,3434 SEER Cancer Statistics Review, 1992-2012 [database on the Internet]. National Cancer Institute. In 2015. Available from: [http://seer.cancer.gov/statfacts/html/stomach.html].
http://seer.cancer.gov/statfacts/html/st...
.
The most effective curative intention treatment for gastric cancer is surgical2525 Norero E, Vargas C, Achurra P, Ceroni M, Mejia R, Martinez C, Muñoz R, Gonzalez P, Calvo A, Díaz A. Survival and perioperative morbidity of totally laparoscopic versus open gastrectomy for early gastric cancer: analysis from a single latin american centre. Arq Bras Cir Dig. 2019;32(1):e1413. doi: 10.1590/0102-672020180001e1413
https://doi.org/10.1590/0102-67202018000...
. Due to the high tumor recurrence rates and poor prognosis, over the past 30 years there has been a strong efforts from the medical community to develop effective cancer therapies - such as chemotherapy and radiotherapy, neoadjuvants or adjuvants - to improve prognosis and long-term survival. Therefore, the treatment of this tumor should be multidisciplinary and individualized. 88 Choi YY, Noh SH, Cheong JH. Evolution of Gastric Cancer Treatment: From the Golden Age of Surgery to an Era of Precision Medicine. Yonsei Med J. 2015;56(5):1177-1185.- doi: 10.3349/ymj.2015.56.5.1177.
https://doi.org/10.3349/ymj.2015.56.5.11...
,1515 Guideline Committee of the Korean Gastric Cancer Association (KGCA), Development Working Group & Review Panel. Korean Practice Guideline for Gastric Cancer 2018: an Evidence-based, Multi-disciplinary Approach. J Gastric Cancer. 2019;19(1):1-48. - doi: 10.5230/jgc.2019.19.e8
https://doi.org/10.5230/jgc.2019.19.e8...
,1919 Japanese Gastric Cancer Association. Japanese gastric cancer treatment guidelines 2010 (ver. 3). Gastric Cancer. 2011;14(2):113-23.- doi: 10.1007/s10120-011-0042-4.
https://doi.org/10.1007/s10120-011-0042-...
,2626 Orditura M, Galizia G, Sforza V, Gambardella V, Fabozzi A, Laterza MM, Andreozzi F, Ventriglia J, Savastano B, Mabilia A, Lieto E, Ciardiello F, De Vita F. Treatment of gastric cancer. World J Gastroenterol. 2014;20(7):1635-1649.- doi: 10.3748/wjg.v20.i7.1635
https://doi.org/10.3748/wjg.v20.i7.1635...
,4040 Xu J, Zhu J, Wei Q. Adjuvant radiochemotherapy versus chemotherapy alone for gastric cancer: Implications for target definition. J Cancer. 2019;10(2):458-466.- doi: 10.1245/s10434-009-0616-0
https://doi.org/10.1245/s10434-009-0616-...
.
Surgical treatment is often the first option, and even when there is no evidence of residual disease during surgery, in most cases there is a need for complementation with some adjuvant therapeutic modality88 Choi YY, Noh SH, Cheong JH. Evolution of Gastric Cancer Treatment: From the Golden Age of Surgery to an Era of Precision Medicine. Yonsei Med J. 2015;56(5):1177-1185.- doi: 10.3349/ymj.2015.56.5.1177.
https://doi.org/10.3349/ymj.2015.56.5.11...
. Histological lymph node invasion, positive peritoneal lavage and local tumor tumors are some of the important prognostic factors for survival3131 Pereira MA, Ramos MFKP, Dias A, Y OKi, Faraj SF, Zilberstein B, Cecconello I, Mello RS, Ribeiro-jr U. Detection of occult lymph node tumor cells in node-negative gastric cancer patients. ABCD Arq Bras Cir Dig. 2017;30(1):30-34.- doi: 10.1590/0102-6720201700010009
https://doi.org/10.1590/0102-67202017000...
.
In 2001, the Intergroup-0116 (INT 0116) clinical trial was published, also known as the MacDonald protocol, which compared two groups of randomized patients, surgical treatment followed by postoperative chemoradiotherapy versus exclusive surgical treatment. The recommended chemotherapy was using 5-fluorouracil, leucovorin and radiotherapy was indicated with the total dose of 4500 cGy2121 Macdonald JS, Smalley SR, Benedetti J, Hundahl SA, Estes NC, Stemmermann GN, Haller DG, Ajani JA, Gunderson LL, Jessup JM, Martenson JA. Chemoradiotherapy after surgery compared with surgery alone for adenocarcinoma of the stomach or gastroesophageal junction. N Engl J Med 2001;345:725-30.- DOI:10.1056/NEJMoa010187
https://doi.org/10.1056/NEJMoa010187...
. The adjuvant protocol showed favorable results and was quickly incorporated as a treatment for gastric cancer in the United States and other western and eastern countries1717 Jácome AA, Sankarankutty AK, Santos JS. Adjuvant therapy for gastric cancer: What have we learned since INT0116?. World J Gastroenterol. 2015;21(13): 3850-3859.- doi: 10.3748/wjg.v21.i13.3850
https://doi.org/10.3748/wjg.v21.i13.3850...
,2020 Kim S, Lim DH, Lee J, Kang WK, MacDonald JS, Park CH, Park SH, Lee SH, Kim K, Park JO, Kim WS, Jung CW, Park YS, Im YH, Sohn TS, Noh JH, Heo JS, Kim YI, Park CK, Park K. An observational study suggesting clinical benefit for adjuvant postoperative chemoradiation in a population of over 500 cases after gastric resection with D2 nodal dissection for adenocarcinoma of the stomach. Int J Radiat Oncol Biol Phys. 2005;63(5):1279-85.- DOI:10.1016/j.ijrobp.2005.05.005
https://doi.org/10.1016/j.ijrobp.2005.05...
,2323 Montenegro P, Flores L, Quintana S, Casanova L, Ruíz E, León J, Mantilla R. Adjuvant chemo radiotherapy after gastrectomy and D2 lymphadenectomy in patients with gastric cancer in the National Institute of Cancer, Lima, Peru. Rev Gastroenterol Peru. 2013;33(1):34-8.- PMID:23539054,3030 Peng J, Wei Y, Zhou F, Dai J, Zhong Y, Xie C, Qin Y, Gong J, Xiong B, Zhou Y. D2-resected stage IIIc gastric cancer patients benefit from adjuvant chemoradiotherapy. Cancer Med. 2016;5(10):2773-2780.- doi: 10.1002/cam4.873.
https://doi.org/10.1002/cam4.873...
,4141 Yakir R, Luna K, Marc W, Tamar S, Avraham R, Ayala H. The toxicity and outcomes of continuous 5-fluorouracil/cisplatin-based chemotherapy followed by chemoradiation in patients with resected high-risk gastric cancer: results of a single institute. Ann Acad Med Singapore. 2008;37(3):200-4.- PMID:18392298. However, only 10% of the study patients underwent D2 lymphadenectomy2121 Macdonald JS, Smalley SR, Benedetti J, Hundahl SA, Estes NC, Stemmermann GN, Haller DG, Ajani JA, Gunderson LL, Jessup JM, Martenson JA. Chemoradiotherapy after surgery compared with surgery alone for adenocarcinoma of the stomach or gastroesophageal junction. N Engl J Med 2001;345:725-30.- DOI:10.1056/NEJMoa010187
https://doi.org/10.1056/NEJMoa010187...
. Thus, there are few studies evaluating the protocol of MacDonald et al.2121 Macdonald JS, Smalley SR, Benedetti J, Hundahl SA, Estes NC, Stemmermann GN, Haller DG, Ajani JA, Gunderson LL, Jessup JM, Martenson JA. Chemoradiotherapy after surgery compared with surgery alone for adenocarcinoma of the stomach or gastroesophageal junction. N Engl J Med 2001;345:725-30.- DOI:10.1056/NEJMoa010187
https://doi.org/10.1056/NEJMoa010187...
in the population of patients undergoing D2 lymphadenectomy, usually employed by some Oncology Services, in the Brazilian population.
The aim of this study was to retrospectively analyze the morbimortality and survival of gastric cancer patients who underwent subtotal or total gastrectomy with D2 lymphadenectomy and who submitted to adjuvant therapy.
METHODS
Medical records of patients with previous diagnosis of advanced gastric adenocarcinoma (noncardia) submitted to surgical treatment with curative intent were selected, treated and followed at the University Hospital of the State University of Campinas, Campinas, SP, Brazil, from January 2002 to August. 2013 and that used the protocol of MacDonald et al. 21, postoperatively.
Adjuvant cancer treatment was started on average 45 days after surgical treatment and consisted of 425 mg/m2 5-fluorouracil associated with leucovorin 20 mg/m2 for five days, followed by radiotherapy 180 cGy/day for five days for five weeks. The radiotherapy period was performed between the third and fourth cycle of chemotherapy. The dose of 5-fluorouracil was changed to 400 mg/m2 and applied on the first four days and last three days of radiotherapy.
A total of 127 cases were identified, with stage IB to IIIC (TNM 2010)33 American Joint Committee on Cancer Staging Manual, 7th, Edge SB, Byrd DR, Compton CC, et al (Eds), Springer, New York 2010. p.117., however were excluded those with compromised resection margin (n=15, 11.8%), distant metastases (n=12, 9.4%), peritoneal implants (n=8, 6.2%) and with death up to 30 days (n=5, - 3.9%). The final number of cases included in the study was 87.
In addition to the analysis of morbidity and mortality, information on epidemiological profile (age and gender), tumor location and histopathology, number of lymph nodes resected and affected, angiolymphatic and perineural invasion, and type of procedure were also obtained.
Statistical analysis
The frequency tables of the categorical variables were made, with absolute (n) and percentage (%) frequency values, and descriptive statistics of numerical variables. Cox regression analysis was used to study survival factors. Kaplan-Meier curves were constructed for survival analysis. The significance level adopted for the study was 5%. The following computer programs were used for statistical analysis: The SAS System for Windows (Statistical Analysis System), version 9.4. SAS Institute Inc, 2002-2008, Cary, NC, USA99 Collett, D. Modelling Survival Data in Medical Research, Chapman & Hall, London, 1994..
RESULTS
The results are summarized in Tables 1 and 2. Depending on the tumor site, subtotal (n=60, 68.9%) or total gastrectomy (n=27, 31.1%) and D2 lymphadenectomy were performed, following the protocol of the Japanese Gastric Cancer Association1818 Japanese Gastric Cancer Association. Japanese classification of gastric carcinoma: 3rd English edition. Gastric Cancer. 2011;14(2):101-12.- doi: 10.1007/s10120-011-0041-5.
https://doi.org/10.1007/s10120-011-0041-...
,1919 Japanese Gastric Cancer Association. Japanese gastric cancer treatment guidelines 2010 (ver. 3). Gastric Cancer. 2011;14(2):113-23.- doi: 10.1007/s10120-011-0042-4.
https://doi.org/10.1007/s10120-011-0042-...
. The predominant tumor location was in the antrum (n=41, 47.1%) which favored the preference for subtotal resection. The average number of resected lymph nodes was 30.8 per patient, considered adequate1818 Japanese Gastric Cancer Association. Japanese classification of gastric carcinoma: 3rd English edition. Gastric Cancer. 2011;14(2):101-12.- doi: 10.1007/s10120-011-0041-5.
https://doi.org/10.1007/s10120-011-0041-...
,1919 Japanese Gastric Cancer Association. Japanese gastric cancer treatment guidelines 2010 (ver. 3). Gastric Cancer. 2011;14(2):113-23.- doi: 10.1007/s10120-011-0042-4.
https://doi.org/10.1007/s10120-011-0042-...
. All were operated at the same institution by the same team of surgeons.
Gender, age range, procedures performed, tumor location and postoperative complications (n=87)
Most patients had tumors at the advanced disease staging - IIIA (n=17, 19.5%), IIIB (n=20, 22.9%) and IIIC (n=23, 26.4%) - totalizing 68.9% of the cases, reflecting the late diagnosis. The most frequent histopathological type was moderately differentiated adenocarcinoma (46%). In addition, 32.1% had both angiolymphatic and perineural invasion (Table 2). Figure 1 shows the overall survival of the 87 patients analyzed.
The risk of death comparing total gastrectomy with subtotal gastrectomy was statistically significant (HR=3.36 CI 95%=1.77-6.40 p=0.0002, Figure 2). Worse outcome also occurred for those with advanced staging and greater lymph node involvement.
The total number of patients who successfully completed the adjuvant protocol was 45 (51.7%). Patients who started the protocol but discontinued due to toxicity, tumor-related worsening, or loss of follow-up were 10 (11.5%), and were considered as incomplete adjuvant. The number of patients who refused or did not start adjuvant treatment was 33 (48.3%).
Patients undergoing adjuvant therapy with complete chemoradiotherapy showed longer survival by the Kaplan-Meier curve when compared to those who received incomplete therapy or underwent exclusive surgery; however the result was not statistically significant (HR=2.09, 95% CI=1.09-4.02, p=0.071, Figure 3). On the other hand, when comparing T4b (IIIB + IIIC) patients who had complete adjuvancy with those undergoing T4b exclusive surgery, there was a statistically significant difference in survival (p=0.004, Figure 4). The study of the group that performed incomplete adjuvancy was impaired by the reduced number of patients.
Survival of the three study groups: complete adjuvant treatment (n=43), incomplete adjuvant treatment (n=10) and surgical treatment only (n=34)
Comparative survival of stage T4b patients (IIIB + IIIC) submitted to adjuvant vs. exclusive operation (p=0.004)
After adjuvant therapy was finished, patients were followed up with frequent outpatient consultations. After two years of surgery the visits were every six months. All patients had clinical follow-up performing abdominal ultrasonography, upper digestive endoscopy, and abdominal, pelvic and chest computed tomography1111 Eom BW, Ryu KW, Lee JH, Choi IJ, Kook MC, Cho SJ, Lee JY, Kim CG, Park SR, Lee JS, Kim YW. Oncologic effectiveness of regular follow-up to detect recurrence after curative resection of gastric cancer. Ann Surg Oncol. 2011;18(2):358.- DOI:10.1056/NEJMoa055531
https://doi.org/10.1056/NEJMoa055531...
.
The main site of recurrence was peritoneum (n=12, 13.7%) and liver (n=10, 11.4%). The presence of tumor recurrence was a predictor of worsening patient survival (HR=2.28, 95% CI=1.08-4.81, p=0.029). Comparing staging III with staging IB + IIA, it was found that staging III showed a statistically significantly shorter survival (RR=2.49 95% CI=1.1163-5.339, p=0.018). The number of lymph nodes affected was also a predictor of poor prognosis (HR=1.174, 95% CI=0.465-2.956, p=0.028) in staging III cases. The other comparisons show no statistically significant difference.
DISCUSSION
The Globocan statistics show that gastric cancer remains important worldwide and was responsible for over 1,000,000 new cases in 2018, with an estimated 73,000 deaths (equivalent to 1 in 12 deaths globally), making it is the fifth most frequently diagnosed and the third leading cause of cancer death. The most common histological type is adenocarcinoma. Among men, it is the most commonly diagnosed tumor and the leading cause of cancer death in many West Asian countries66 Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394-424. - doi: 10.3322/caac.21492.
Surgical resection followed by adequate lymphadenectomy and detailed analysis of resected lymph nodes remains the best chance of disease control and cure, in early cases. Despite improvements in surgical techniques and more extensive lymphadenectomy, 40% to 60% of patients relapse from 2 to 5 years. Therefore, even when performing R0 surgical resection, there is improvement with the addition of chemotherapy and radiotherapy, necessary and indispensable for increased survival1414 Giampieri R, Del Prete M, Cantini L, Baleani MG, Bittoni A, Maccaroni E, Berardi R. Optimal management of resected gastric cancer. Cancer Manag Res. 2018;10:1605-1618.- doi: 10.2147/CMAR.S151552
https://doi.org/10.2147/CMAR.S151552...
,3131 Pereira MA, Ramos MFKP, Dias A, Y OKi, Faraj SF, Zilberstein B, Cecconello I, Mello RS, Ribeiro-jr U. Detection of occult lymph node tumor cells in node-negative gastric cancer patients. ABCD Arq Bras Cir Dig. 2017;30(1):30-34.- doi: 10.1590/0102-6720201700010009
https://doi.org/10.1590/0102-67202017000...
.
The conversion therapy has recently emerged as an alternative therapy, prolonging survival in patients with advanced neoplastic disease. It consists of oncologic treatments followed by surgery in stage IV patients. It is an option to treat unresectable lesions in patients with distant lymph node metastasis and even with metastatic disease or peritoneal dissemination3232 Ramos MFKP, Pereira MA, Charruf AZ, Dias AR, Castria TB, Barchi LC, Ribeiro-Júnior U, Zilberstein B, Cecconello I. Conversion therapy for gastric cancer: expanding the treatment possibilities. Arq Bras Cir Dig. 2019;32(2):e1435. - doi: 10.1590/0102-672020190001e1435
https://doi.org/10.1590/0102-67202019000...
.
Despite major debates over the past 30 years regarding what would be the best surgical technique and extension of lymphadenectomy, it is currently accepted that resection to D2 yields the best long-term results regarding tumor survival and recurrence. The vast majority of recent large clinical trials perform D2 lymphadenectomy as the basis for curative surgery2222 Mogal H, Fields R, Maithel SK, Votanopoulos K. In Patients with Localized and Resectable Gastric Cancer, What is the Optimal Extent of Lymph Node Dissection-D1 Versus D2 Versus D3? Ann Surg Oncol. 2019 May 10. doi: 10.1245/s10434-019-07417-5. [Epub ahead of print],2727 Pacelli F, Papa V, Rosa F, Tortorelli AP, Sanchez AM, Covino M, Bossola M, Doglietto GB. Four Hundred Consecutive Total Gastrectomies for Gastric Cancer. A Single-Institution Experience. Arch Surg. 2008;143(8):769-75.- doi: 10.1001/archsurg.143.8.769
https://doi.org/10.1001/archsurg.143.8.7...
,3636 Songun I, Putter H, Kranenbarg EM, Sasako M, van de Velde CJ. Surgical treatment of gastric cancer: 15-year follow-up results of the randomised nationwide Dutch D1D2 trial. Lancet Oncol. 2010;11(5):439-49.- doi: 10.1016/S1470-2045(10)70070-X
https://doi.org/10.1016/S1470-2045(10)70...
. It is also agreed that the presence of microscopically affected margins is an independent prognostic factor3939 Wang SY, Yeh CN, Lee HL, Liu YY, Chao TC, Hwang TL, Jan YY, Chen MF. Clinical impact of positive surgical margin status on gastric cancer patients undergoing gastrectomy. Ann Surg Oncol. 2009;16(10):2738-43. - doi: 10.1245/s10434-009-0616-0
https://doi.org/10.1245/s10434-009-0616-...
.
The oncologic treatments, neoadjuvant, perioperative or adjuvant, vary considerably and specialists employ various regimens to effectively control the disease. Presently, there is no consensus on which one is most appropriate, considering that the studies performed were heterogeneously designed with different drugs and dose regimens, including chemotherapy alone or in combination with radiotherapy1515 Guideline Committee of the Korean Gastric Cancer Association (KGCA), Development Working Group & Review Panel. Korean Practice Guideline for Gastric Cancer 2018: an Evidence-based, Multi-disciplinary Approach. J Gastric Cancer. 2019;19(1):1-48. - doi: 10.5230/jgc.2019.19.e8
https://doi.org/10.5230/jgc.2019.19.e8...
,1919 Japanese Gastric Cancer Association. Japanese gastric cancer treatment guidelines 2010 (ver. 3). Gastric Cancer. 2011;14(2):113-23.- doi: 10.1007/s10120-011-0042-4.
https://doi.org/10.1007/s10120-011-0042-...
,2626 Orditura M, Galizia G, Sforza V, Gambardella V, Fabozzi A, Laterza MM, Andreozzi F, Ventriglia J, Savastano B, Mabilia A, Lieto E, Ciardiello F, De Vita F. Treatment of gastric cancer. World J Gastroenterol. 2014;20(7):1635-1649.- doi: 10.3748/wjg.v20.i7.1635
https://doi.org/10.3748/wjg.v20.i7.1635...
,4040 Xu J, Zhu J, Wei Q. Adjuvant radiochemotherapy versus chemotherapy alone for gastric cancer: Implications for target definition. J Cancer. 2019;10(2):458-466.- doi: 10.1245/s10434-009-0616-0
https://doi.org/10.1245/s10434-009-0616-...
.
The most important studies including neoadjuvant chemotherapy followed by surgery, well controlled and with long follow-up were MAGIC1010 Cunningham D, Allum WH, Stenning SP, et al. Perioperative chemotherapy versus surgery alone for resectable gastroesophageal cancer. N Engl J Med. 2006;355(1):11-20.- DOI:10.1056/NEJMoa055531
https://doi.org/10.1056/NEJMoa055531...
, FFCD 97034242 Ychou M, Boige V, Pignon J-P, Conroy T, Bouché O, Lebreton G, Ducourtieux M, Bedenne L, Fabre JM, Saint-Aubert B, Genève J, Lasser P, Rougier P. Perioperative chemotherapy compared with surgery alone for resectable gastroesophageal adenocarcinoma: an FNCLCC and FFCD multicenter phase III trial. J Clin Oncol. 2011;29(13):1715-1721.- doi: 10.1200/JCO.2010.33.0597
https://doi.org/10.1200/JCO.2010.33.0597...
and FLOT-411 Al-Batran SE, Homann N, Pauligk C, Goetze TO, Meiler J, Kasper S, Kopp HG, Mayer F, Haag GM, Luley K, Lindig U, Schmiegel W, Pohl M, Stoehlmacher J, Folprecht G, Probst S, Prasnikar N, Fischbach W, Mahlberg R, Trojan J, Koenigsmann M, Martens UM, Thuss-Patience P, Egger M, Block A, Heinemann V, Illerhaus G, Moehler M, Schenk M, Kullmann F, Behringer DM, Heike M, Pink D, Teschendorf C, Löhr C, Bernhard H, Schuch G, Rethwisch V, von Weikersthal LF, Hartmann JT, Kneba M, Daum S, Schulmann K, Weniger J, Belle S, Gaiser T, Oduncu FS, Güntner M, Hozaeel W, Reichart A, Jäger E, Kraus T, Mönig S, Bechstein WO, Schuler M, Schmalenberg H, Hofheinz RD; FLOT4-AIO Investigators. Perioperative chemotherapy with fluorouracil plus leucovorin, oxaliplatin, and docetaxel versus fluorouracil or capecitabine plus cisplatin and epirubicin for locally advanced, resectable gastric or gastro-oesophageal junction adenocarcinoma (FLOT4): a randomised, phase 2/3 trial. Lancet. 2019;393(10184):1948-1957 - doi: 10.1016/S0140-6736(18)32557-1
https://doi.org/10.1016/S0140-6736(18)32...
. Interestingly, most adjuvant chemotherapy treatment studies are in Asian and include ACTS-GC3333 Sasako M, Sakuramoto S, Katai H, Kinoshita T, Furukawa H, Yamaguchi T, Nashimoto A, Fujii M, Nakajima T, Ohashi Y. Five-year outcomes of a randomized phase III trial comparing adjuvant chemotherapy with S-1 versus surgery alone in stage II or III gastric cancer. J Clin Oncol. 2011;29(33):4387-4393.- doi: 10.1200/JCO.2011.36.5908
https://doi.org/10.1200/JCO.2011.36.5908...
, CLASSIC2424 Noh SH, Park SR, Yang H-K, et al. Adjuvant capecitabine plus oxaliplatin for gastric cancer after D2 gastrectomy (CLASSIC): 5-year follow-up of an open-label, randomised phase 3 trial. Lancet Oncol. 2014;15(12):1389-1396.- doi: 10.1016/S1470-2045(14)70473-5.
https://doi.org/10.1016/S1470-2045(14)70...
, SAMIT3838 Tsuburaya A, Yoshida K, Kobayashi M, Yoshino S, Takahashi M, Takiguchi N, Tanabe K, Takahashi N, Imamura H, Tatsumoto N1, Hara A, Nishikawa K, Fukushima R, Nozaki I, Kojima H, Miyashita Y, Oba K, Buyse M, Morita S, Sakamoto J. Sequential paclitaxel followed by tegafur and uracil (UFT) or S-1 versus UFT or S-1 monotherapy as adjuvant chemotherapy for T4a/b gastric cancer (SAMIT): a phase 3 factorial randomised controlled trial. Lancet Oncol. 2014;15(8):886-893.- doi: 10.1016/S1470-2045(14)70025-7
https://doi.org/10.1016/S1470-2045(14)70...
and ITACA-S11 Al-Batran SE, Homann N, Pauligk C, Goetze TO, Meiler J, Kasper S, Kopp HG, Mayer F, Haag GM, Luley K, Lindig U, Schmiegel W, Pohl M, Stoehlmacher J, Folprecht G, Probst S, Prasnikar N, Fischbach W, Mahlberg R, Trojan J, Koenigsmann M, Martens UM, Thuss-Patience P, Egger M, Block A, Heinemann V, Illerhaus G, Moehler M, Schenk M, Kullmann F, Behringer DM, Heike M, Pink D, Teschendorf C, Löhr C, Bernhard H, Schuch G, Rethwisch V, von Weikersthal LF, Hartmann JT, Kneba M, Daum S, Schulmann K, Weniger J, Belle S, Gaiser T, Oduncu FS, Güntner M, Hozaeel W, Reichart A, Jäger E, Kraus T, Mönig S, Bechstein WO, Schuler M, Schmalenberg H, Hofheinz RD; FLOT4-AIO Investigators. Perioperative chemotherapy with fluorouracil plus leucovorin, oxaliplatin, and docetaxel versus fluorouracil or capecitabine plus cisplatin and epirubicin for locally advanced, resectable gastric or gastro-oesophageal junction adenocarcinoma (FLOT4): a randomised, phase 2/3 trial. Lancet. 2019;393(10184):1948-1957 - doi: 10.1016/S0140-6736(18)32557-1
https://doi.org/10.1016/S0140-6736(18)32...
.
To reduce the likelihood of local recurrence of resected gastric cancer, in addition to adjuvant chemotherapy, local treatments employing radiotherapy have been investigated in both neoadjuvant and adjuvant contexts. Thus, the studies that best evaluated this treatment were: INT 01162121 Macdonald JS, Smalley SR, Benedetti J, Hundahl SA, Estes NC, Stemmermann GN, Haller DG, Ajani JA, Gunderson LL, Jessup JM, Martenson JA. Chemoradiotherapy after surgery compared with surgery alone for adenocarcinoma of the stomach or gastroesophageal junction. N Engl J Med 2001;345:725-30.- DOI:10.1056/NEJMoa010187
https://doi.org/10.1056/NEJMoa010187...
, ARTIST2828 Park SH, Sohn TS, Lee J, Lim DH, Hong ME, Kim KM, Sohn I, Jung SH, Choi MG, Lee JH1, Bae JM, Kim S, Kim ST, Park JO, Park YS, Lim HY, Kang WK. Phase III trial to compare adjuvant chemotherapy with capecitabine and cisplatin versus concurrent chemoradiotherapy in gastric cancer: final report of the adjuvant chemoradiotherapy in stomach tumors trial, including survival and subset analyses. J Clin Oncol. 2015;33(28):3130-3136.- doi: 10.1200/JCO.2014.58.3930
https://doi.org/10.1200/JCO.2014.58.3930...
, POET3737 Stahl M, Walz MK, Stuschke M, Lehmann N, Meyer HJ, Riera-Knorrenschild J, Langer P, Engenhart-Cabillic R, Bitzer M, Königsrainer A, Budach W, Wilke H. Phase III comparison of preoperative chemotherapy compared with chemoradiotherapy in patients with locally advanced adenocarcinoma of the esophagogastric junction. J Clin Oncol. 2009;27(6):851-856.- doi: 10.1200/JCO.2008.17.0506
https://doi.org/10.1200/JCO.2008.17.0506...
and CROSS1616 van Hagen P, Hulshof MC, van Lanschot JJ, Steyerberg EW, van Berge Henegouwen MI, Wijnhoven BP, Richel DJ, Nieuwenhuijzen GA, Hospers GA, Bonenkamp JJ, Cuesta MA, Blaisse RJ, Busch OR, ten Kate FJ, Creemers GJ, Punt CJ, Plukker JT, Verheul HM, Spillenaar Bilgen EJ, van Dekken H, van der Sangen MJ, Rozema T, Biermann K, Beukema JC, Piet AH, van Rij CM, Reinders JG, Tilanus HW, van der Gaast A; CROSS Group. Preoperative chemoradiotherapy for esophageal or junctional cancer. N Engl J Med. 2012;366(22):2074-2084.- doi: 10.1056/NEJMoa1112088.
https://doi.org/10.1056/NEJMoa1112088...
.
The INT-0116 study, which established postoperative chemoradiotherapy treatment using 5-fluorouracil, leucovorin and a total dose of 4500 cGy, showed the benefit for patients into the T2N0 staging, which according to the classification included tumors involving the subserosa and muscularis propria, respectively (which would be classified as T3 and T2, according to the current TNM 2010 classification). This study showed a three-year survival rate of 50% in the group receiving chemoradiotherapy vs. 41% in the exclusive surgery treated group (p=0.005) and progression-free survival rate of 48% in the chemoradiotherapy group vs. 31% in the exclusive surgery treated group (p<0.001)2121 Macdonald JS, Smalley SR, Benedetti J, Hundahl SA, Estes NC, Stemmermann GN, Haller DG, Ajani JA, Gunderson LL, Jessup JM, Martenson JA. Chemoradiotherapy after surgery compared with surgery alone for adenocarcinoma of the stomach or gastroesophageal junction. N Engl J Med 2001;345:725-30.- DOI:10.1056/NEJMoa010187
https://doi.org/10.1056/NEJMoa010187...
. Smalley et al.35 in 2012 also demonstrated that the benefits of chemoradiotherapy remained after 10 years of postoperative follow-up and that the results remained favorable in relation to mortality and tumor recurrence.
In this research were selected and included patients from staging T2N0 (IB) and those with any lymph node involvement, in order to make a similar selection to the original article, without esophagogastric junction tumors included. Eighty-seven patients with complete 5-year follow-up were included in the present study, however only 49.1% completed all treatment, 11.5% started treatment and discontinued due to severe side effects and 39.1% did not start the protocol for lack of clinical conditions. Statistical analysis failed to show benefit in terms of survival gain for patients undergoing complete adjuvant treatment considering all stages, although the Kaplan-Meier curve in this group showed a difference in mean survival when comparing patients that performed adjuvant therapy with those who did not (73.26 vs. 38.58 months respectively, Figure 3). It is possible that with a larger sample, the benefit of adjuvant therapy may be statistically significant. On the other hand, when comparing only patiens with T4b staging (IIIB + IIIC) who underwent adjuvant treatment or not, survival gain was demonstrated (Figure 4). Our results also show a statistically significant survival gain in patients undergoing subtotal gastrectomy compared with total gastrectomy (Figure 2). Therefore, as already shown in the literature, there is a significant increase in morbidity when comparing total with subtotal gastrectomy results. Whenever possible, subtotal gastrectomy is preferable, with the surgical margins preserved44 Andreollo NA, Lopes LR, Coelho Neto JS. Postoperative complications after total gastrectomy in the gastric cancer. Analysis of 300 patients. ABCD Arq Bras Cir Dig. 2011;24(2):126-130 - doi:10.1590/S0102-67202011000200007.
https://doi.org/10.1590/S0102-6720201100...
,2727 Pacelli F, Papa V, Rosa F, Tortorelli AP, Sanchez AM, Covino M, Bossola M, Doglietto GB. Four Hundred Consecutive Total Gastrectomies for Gastric Cancer. A Single-Institution Experience. Arch Surg. 2008;143(8):769-75.- doi: 10.1001/archsurg.143.8.769
https://doi.org/10.1001/archsurg.143.8.7...
.
In addition, patients in staging I and II compared to staging III who did not have recurrence of tumor in the peritoneum and liver when compared to patients who had this type of recurrence, and patients in staging III who did not have lymph nodes involvement compared to patients who had lymph nodes involvement, also had survival gains. The other comparisons did not show statistically significant differences.
The related criticism about the study by MacDonald et al. 21 was that only 10% of patients (n=556) underwent a D2 resection3737 Stahl M, Walz MK, Stuschke M, Lehmann N, Meyer HJ, Riera-Knorrenschild J, Langer P, Engenhart-Cabillic R, Bitzer M, Königsrainer A, Budach W, Wilke H. Phase III comparison of preoperative chemotherapy compared with chemoradiotherapy in patients with locally advanced adenocarcinoma of the esophagogastric junction. J Clin Oncol. 2009;27(6):851-856.- doi: 10.1200/JCO.2008.17.0506
https://doi.org/10.1200/JCO.2008.17.0506...
. This fact raised doubts regarding the real need for radiotherapy for those undergoing radical resection. Another negative aspect is its toxicity, hematologic toxicity can reach 54% and gastrointestinal toxicity in 33% of patients, with a treatment-related mortality of 1%1717 Jácome AA, Sankarankutty AK, Santos JS. Adjuvant therapy for gastric cancer: What have we learned since INT0116?. World J Gastroenterol. 2015;21(13): 3850-3859.- doi: 10.3748/wjg.v21.i13.3850
https://doi.org/10.3748/wjg.v21.i13.3850...
.
Similar studies using the same adjuvant protocol reported satisfactory results. Kim et al.2020 Kim S, Lim DH, Lee J, Kang WK, MacDonald JS, Park CH, Park SH, Lee SH, Kim K, Park JO, Kim WS, Jung CW, Park YS, Im YH, Sohn TS, Noh JH, Heo JS, Kim YI, Park CK, Park K. An observational study suggesting clinical benefit for adjuvant postoperative chemoradiation in a population of over 500 cases after gastric resection with D2 nodal dissection for adenocarcinoma of the stomach. Int J Radiat Oncol Biol Phys. 2005;63(5):1279-85.- DOI:10.1016/j.ijrobp.2005.05.005
https://doi.org/10.1016/j.ijrobp.2005.05...
employed this protocol in 544 patients undergoing curative treatment and D2 lymphadenectomy, concluding that 5-year survival rates were consistently longer in stages II, IIIA, IIIB and IV than in the group of 446 patients undergoing exclusive surgery. In addition, the adjuvant treatment employed was associated with increases in median duration of relapse-free survival. Yakir et al.4141 Yakir R, Luna K, Marc W, Tamar S, Avraham R, Ayala H. The toxicity and outcomes of continuous 5-fluorouracil/cisplatin-based chemotherapy followed by chemoradiation in patients with resected high-risk gastric cancer: results of a single institute. Ann Acad Med Singapore. 2008;37(3):200-4.- PMID:18392298 employed the same protocol in 36 staging T4b patients, concluding that median disease-free survival was 37.4 months and overall survival was 40.3 months, with no deaths related to treatment toxicity. Montenegro et al.2323 Montenegro P, Flores L, Quintana S, Casanova L, Ruíz E, León J, Mantilla R. Adjuvant chemo radiotherapy after gastrectomy and D2 lymphadenectomy in patients with gastric cancer in the National Institute of Cancer, Lima, Peru. Rev Gastroenterol Peru. 2013;33(1):34-8.- PMID:23539054 used the same protocol in 84 patients with advanced gastric adenocarcinoma who underwent gastric resection and D2 lymphadenectomy, concluding that the average 3-year survival was 23.9%; however, analyzing the groups for lymph node invasion, they found that in the same period, N1 survival was 100%, N2 was 51.9% and N3 was 16.3%. They conclude that the adjuvant protocol used reduced the risk of death and relapse to three years, especially in patients with positive N1-N2 lymph nodes who underwent curative resection with D2 lymphadenectomy, but recurrence was more frequent in positive N3 lymph nodes and suggest employ new adjuvant protocols in this group of patients to decrease relapse rates. Favacho et al.1212 Favacho BC, Costa Cda S, Magalhães TC, de Assumpção PP, Ishak G. T4b gastric carcinoma: 12 years of experience at an University Hospital. Arq Bras Cir Dig. 2013;26(4):268-73.- dói: 10.1590/S0102-67202013000400004. analyzed 27 patients with staging T4b advanced gastric cancer who were only submitted to surgical treatment without adjuvant therapy and reported a 6-month survival of 63.27%.
In our opinion, for a better evaluation of the response of adjuvant chemoradiotherapy treatment, it is important to eliminate factors that may modify or create prognostic biases in the selected sample. Dosages of biomarkers such as HER2, microsatellite instability, Epstein-Barr virus, PD-L1 dosage and other markers may contribute to open new treatments and survival analysis, which associated with chemoradiotherapy, contribute to increased survival2929 Norero E, Vargas C, Achurra P, Ceroni M, Mejia R, Martinez C, Muñoz R, Gonzalez P, Calvo A, Díaz A. Survival and perioperative morbidity of totally laparoscopic versus open gastrectomy for early gastric cancer: analysis from a single latin american centre. Arq Bras Cir Dig. 2019;32(1):e1413. doi: 10.1590/0102-672020180001e1413
https://doi.org/10.1590/0102-67202018000...
.
Therefore, it should be emphasized that the treatment of gastric cancer is necessarily multidisciplinary22 Alves LB, Tsukazan MT, Serafim AE, Mendoza R, Padoin AV, Baú PC, Moreira LF. Prognostic value of carcinoembryonic antigen levels in transoperative peritoneal lavage in patients with gastric cancer. Arq Bras Cir Dig. 2018;31(1):e1358 - doi: 10.1590/0102-672020180001e1358.
https://doi.org/10.1590/0102-67202018000...
,1515 Guideline Committee of the Korean Gastric Cancer Association (KGCA), Development Working Group & Review Panel. Korean Practice Guideline for Gastric Cancer 2018: an Evidence-based, Multi-disciplinary Approach. J Gastric Cancer. 2019;19(1):1-48. - doi: 10.5230/jgc.2019.19.e8
https://doi.org/10.5230/jgc.2019.19.e8...
and the survival analysis of the series suggests that the chemoradiation protocol proposed by Macdonald et al.2121 Macdonald JS, Smalley SR, Benedetti J, Hundahl SA, Estes NC, Stemmermann GN, Haller DG, Ajani JA, Gunderson LL, Jessup JM, Martenson JA. Chemoradiotherapy after surgery compared with surgery alone for adenocarcinoma of the stomach or gastroesophageal junction. N Engl J Med 2001;345:725-30.- DOI:10.1056/NEJMoa010187
https://doi.org/10.1056/NEJMoa010187...
may have benefits for patients with advanced disease undergoing surgery with curative intent and D2 lymphadenectomy. Additional studies with similar design are needed to define the real benefit of adjuvant chemoradiotherapy for the treatment of advanced gastric cancer.
CONCLUSION
Adjuvant chemoradiotherapy presents survival gain for T4b patients undergoing surgical treatment with curative intent.
REFERENCES
-
1Al-Batran SE, Homann N, Pauligk C, Goetze TO, Meiler J, Kasper S, Kopp HG, Mayer F, Haag GM, Luley K, Lindig U, Schmiegel W, Pohl M, Stoehlmacher J, Folprecht G, Probst S, Prasnikar N, Fischbach W, Mahlberg R, Trojan J, Koenigsmann M, Martens UM, Thuss-Patience P, Egger M, Block A, Heinemann V, Illerhaus G, Moehler M, Schenk M, Kullmann F, Behringer DM, Heike M, Pink D, Teschendorf C, Löhr C, Bernhard H, Schuch G, Rethwisch V, von Weikersthal LF, Hartmann JT, Kneba M, Daum S, Schulmann K, Weniger J, Belle S, Gaiser T, Oduncu FS, Güntner M, Hozaeel W, Reichart A, Jäger E, Kraus T, Mönig S, Bechstein WO, Schuler M, Schmalenberg H, Hofheinz RD; FLOT4-AIO Investigators. Perioperative chemotherapy with fluorouracil plus leucovorin, oxaliplatin, and docetaxel versus fluorouracil or capecitabine plus cisplatin and epirubicin for locally advanced, resectable gastric or gastro-oesophageal junction adenocarcinoma (FLOT4): a randomised, phase 2/3 trial. Lancet. 2019;393(10184):1948-1957 - doi: 10.1016/S0140-6736(18)32557-1
» https://doi.org/10.1016/S0140-6736(18)32557-1 -
2Alves LB, Tsukazan MT, Serafim AE, Mendoza R, Padoin AV, Baú PC, Moreira LF. Prognostic value of carcinoembryonic antigen levels in transoperative peritoneal lavage in patients with gastric cancer. Arq Bras Cir Dig. 2018;31(1):e1358 - doi: 10.1590/0102-672020180001e1358.
» https://doi.org/10.1590/0102-672020180001e1358 -
3American Joint Committee on Cancer Staging Manual, 7th, Edge SB, Byrd DR, Compton CC, et al (Eds), Springer, New York 2010. p.117.
-
4Andreollo NA, Lopes LR, Coelho Neto JS. Postoperative complications after total gastrectomy in the gastric cancer. Analysis of 300 patients. ABCD Arq Bras Cir Dig. 2011;24(2):126-130 - doi:10.1590/S0102-67202011000200007.
» https://doi.org/10.1590/S0102-67202011000200007 -
5Bajetta E, Floriani I, Di Bartolomeo M, et al. Randomized trial on adjuvant treatment with FOLFIRI followed by docetaxel and cisplatin versus 5-fluorouracil and folinic acid for radically resected gastric cancer. Ann Oncol. 2014;25(7):1373-1378. - doi:10.1093/annonc/mdu146
» https://doi.org/10.1093/annonc/mdu146 -
6Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394-424. - doi: 10.3322/caac.21492
-
7Brazil, Ministry of Health National Cancer Institute. [database on the Internet]. In 2018. Available from: https://www.inca.gov.br/tipos-de-cancer/cancer-de-estomago
» https://www.inca.gov.br/tipos-de-cancer/cancer-de-estomago -
8Choi YY, Noh SH, Cheong JH. Evolution of Gastric Cancer Treatment: From the Golden Age of Surgery to an Era of Precision Medicine. Yonsei Med J. 2015;56(5):1177-1185.- doi: 10.3349/ymj.2015.56.5.1177.
» https://doi.org/10.3349/ymj.2015.56.5.1177 -
9Collett, D. Modelling Survival Data in Medical Research, Chapman & Hall, London, 1994.
-
10Cunningham D, Allum WH, Stenning SP, et al. Perioperative chemotherapy versus surgery alone for resectable gastroesophageal cancer. N Engl J Med. 2006;355(1):11-20.- DOI:10.1056/NEJMoa055531
» https://doi.org/10.1056/NEJMoa055531 -
11Eom BW, Ryu KW, Lee JH, Choi IJ, Kook MC, Cho SJ, Lee JY, Kim CG, Park SR, Lee JS, Kim YW. Oncologic effectiveness of regular follow-up to detect recurrence after curative resection of gastric cancer. Ann Surg Oncol. 2011;18(2):358.- DOI:10.1056/NEJMoa055531
» https://doi.org/10.1056/NEJMoa055531 -
12Favacho BC, Costa Cda S, Magalhães TC, de Assumpção PP, Ishak G. T4b gastric carcinoma: 12 years of experience at an University Hospital. Arq Bras Cir Dig. 2013;26(4):268-73.- dói: 10.1590/S0102-67202013000400004.
-
13Ferlay J, Soerjomataram I, Dikshit R, Eser S, Mathers C, Rebelo M, Parkin DM, Forman D, Bray F. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015;136: E359-86.- doi: 10.1002/ijc.29210.
» https://doi.org/10.1002/ijc.29210 -
14Giampieri R, Del Prete M, Cantini L, Baleani MG, Bittoni A, Maccaroni E, Berardi R. Optimal management of resected gastric cancer. Cancer Manag Res. 2018;10:1605-1618.- doi: 10.2147/CMAR.S151552
» https://doi.org/10.2147/CMAR.S151552 -
15Guideline Committee of the Korean Gastric Cancer Association (KGCA), Development Working Group & Review Panel. Korean Practice Guideline for Gastric Cancer 2018: an Evidence-based, Multi-disciplinary Approach. J Gastric Cancer. 2019;19(1):1-48. - doi: 10.5230/jgc.2019.19.e8
» https://doi.org/10.5230/jgc.2019.19.e8 -
16van Hagen P, Hulshof MC, van Lanschot JJ, Steyerberg EW, van Berge Henegouwen MI, Wijnhoven BP, Richel DJ, Nieuwenhuijzen GA, Hospers GA, Bonenkamp JJ, Cuesta MA, Blaisse RJ, Busch OR, ten Kate FJ, Creemers GJ, Punt CJ, Plukker JT, Verheul HM, Spillenaar Bilgen EJ, van Dekken H, van der Sangen MJ, Rozema T, Biermann K, Beukema JC, Piet AH, van Rij CM, Reinders JG, Tilanus HW, van der Gaast A; CROSS Group. Preoperative chemoradiotherapy for esophageal or junctional cancer. N Engl J Med. 2012;366(22):2074-2084.- doi: 10.1056/NEJMoa1112088.
» https://doi.org/10.1056/NEJMoa1112088 -
17Jácome AA, Sankarankutty AK, Santos JS. Adjuvant therapy for gastric cancer: What have we learned since INT0116?. World J Gastroenterol. 2015;21(13): 3850-3859.- doi: 10.3748/wjg.v21.i13.3850
» https://doi.org/10.3748/wjg.v21.i13.3850 -
18Japanese Gastric Cancer Association. Japanese classification of gastric carcinoma: 3rd English edition. Gastric Cancer. 2011;14(2):101-12.- doi: 10.1007/s10120-011-0041-5.
» https://doi.org/10.1007/s10120-011-0041-5 -
19Japanese Gastric Cancer Association. Japanese gastric cancer treatment guidelines 2010 (ver. 3). Gastric Cancer. 2011;14(2):113-23.- doi: 10.1007/s10120-011-0042-4.
» https://doi.org/10.1007/s10120-011-0042-4 -
20Kim S, Lim DH, Lee J, Kang WK, MacDonald JS, Park CH, Park SH, Lee SH, Kim K, Park JO, Kim WS, Jung CW, Park YS, Im YH, Sohn TS, Noh JH, Heo JS, Kim YI, Park CK, Park K. An observational study suggesting clinical benefit for adjuvant postoperative chemoradiation in a population of over 500 cases after gastric resection with D2 nodal dissection for adenocarcinoma of the stomach. Int J Radiat Oncol Biol Phys. 2005;63(5):1279-85.- DOI:10.1016/j.ijrobp.2005.05.005
» https://doi.org/10.1016/j.ijrobp.2005.05.005 -
21Macdonald JS, Smalley SR, Benedetti J, Hundahl SA, Estes NC, Stemmermann GN, Haller DG, Ajani JA, Gunderson LL, Jessup JM, Martenson JA. Chemoradiotherapy after surgery compared with surgery alone for adenocarcinoma of the stomach or gastroesophageal junction. N Engl J Med 2001;345:725-30.- DOI:10.1056/NEJMoa010187
» https://doi.org/10.1056/NEJMoa010187 -
22Mogal H, Fields R, Maithel SK, Votanopoulos K. In Patients with Localized and Resectable Gastric Cancer, What is the Optimal Extent of Lymph Node Dissection-D1 Versus D2 Versus D3? Ann Surg Oncol. 2019 May 10. doi: 10.1245/s10434-019-07417-5. [Epub ahead of print]
-
23Montenegro P, Flores L, Quintana S, Casanova L, Ruíz E, León J, Mantilla R. Adjuvant chemo radiotherapy after gastrectomy and D2 lymphadenectomy in patients with gastric cancer in the National Institute of Cancer, Lima, Peru. Rev Gastroenterol Peru. 2013;33(1):34-8.- PMID:23539054
-
24Noh SH, Park SR, Yang H-K, et al. Adjuvant capecitabine plus oxaliplatin for gastric cancer after D2 gastrectomy (CLASSIC): 5-year follow-up of an open-label, randomised phase 3 trial. Lancet Oncol. 2014;15(12):1389-1396.- doi: 10.1016/S1470-2045(14)70473-5.
» https://doi.org/10.1016/S1470-2045(14)70473-5 -
25Norero E, Vargas C, Achurra P, Ceroni M, Mejia R, Martinez C, Muñoz R, Gonzalez P, Calvo A, Díaz A. Survival and perioperative morbidity of totally laparoscopic versus open gastrectomy for early gastric cancer: analysis from a single latin american centre. Arq Bras Cir Dig. 2019;32(1):e1413. doi: 10.1590/0102-672020180001e1413
» https://doi.org/10.1590/0102-672020180001e1413 -
26Orditura M, Galizia G, Sforza V, Gambardella V, Fabozzi A, Laterza MM, Andreozzi F, Ventriglia J, Savastano B, Mabilia A, Lieto E, Ciardiello F, De Vita F. Treatment of gastric cancer. World J Gastroenterol. 2014;20(7):1635-1649.- doi: 10.3748/wjg.v20.i7.1635
» https://doi.org/10.3748/wjg.v20.i7.1635 -
27Pacelli F, Papa V, Rosa F, Tortorelli AP, Sanchez AM, Covino M, Bossola M, Doglietto GB. Four Hundred Consecutive Total Gastrectomies for Gastric Cancer. A Single-Institution Experience. Arch Surg. 2008;143(8):769-75.- doi: 10.1001/archsurg.143.8.769
» https://doi.org/10.1001/archsurg.143.8.769 -
28Park SH, Sohn TS, Lee J, Lim DH, Hong ME, Kim KM, Sohn I, Jung SH, Choi MG, Lee JH1, Bae JM, Kim S, Kim ST, Park JO, Park YS, Lim HY, Kang WK. Phase III trial to compare adjuvant chemotherapy with capecitabine and cisplatin versus concurrent chemoradiotherapy in gastric cancer: final report of the adjuvant chemoradiotherapy in stomach tumors trial, including survival and subset analyses. J Clin Oncol. 2015;33(28):3130-3136.- doi: 10.1200/JCO.2014.58.3930
» https://doi.org/10.1200/JCO.2014.58.3930 -
29Norero E, Vargas C, Achurra P, Ceroni M, Mejia R, Martinez C, Muñoz R, Gonzalez P, Calvo A, Díaz A. Survival and perioperative morbidity of totally laparoscopic versus open gastrectomy for early gastric cancer: analysis from a single latin american centre. Arq Bras Cir Dig. 2019;32(1):e1413. doi: 10.1590/0102-672020180001e1413
» https://doi.org/10.1590/0102-672020180001e1413 -
30Peng J, Wei Y, Zhou F, Dai J, Zhong Y, Xie C, Qin Y, Gong J, Xiong B, Zhou Y. D2-resected stage IIIc gastric cancer patients benefit from adjuvant chemoradiotherapy. Cancer Med. 2016;5(10):2773-2780.- doi: 10.1002/cam4.873.
» https://doi.org/10.1002/cam4.873 -
31Pereira MA, Ramos MFKP, Dias A, Y OKi, Faraj SF, Zilberstein B, Cecconello I, Mello RS, Ribeiro-jr U. Detection of occult lymph node tumor cells in node-negative gastric cancer patients. ABCD Arq Bras Cir Dig. 2017;30(1):30-34.- doi: 10.1590/0102-6720201700010009
» https://doi.org/10.1590/0102-6720201700010009 -
32Ramos MFKP, Pereira MA, Charruf AZ, Dias AR, Castria TB, Barchi LC, Ribeiro-Júnior U, Zilberstein B, Cecconello I. Conversion therapy for gastric cancer: expanding the treatment possibilities. Arq Bras Cir Dig. 2019;32(2):e1435. - doi: 10.1590/0102-672020190001e1435
» https://doi.org/10.1590/0102-672020190001e1435 -
33Sasako M, Sakuramoto S, Katai H, Kinoshita T, Furukawa H, Yamaguchi T, Nashimoto A, Fujii M, Nakajima T, Ohashi Y. Five-year outcomes of a randomized phase III trial comparing adjuvant chemotherapy with S-1 versus surgery alone in stage II or III gastric cancer. J Clin Oncol. 2011;29(33):4387-4393.- doi: 10.1200/JCO.2011.36.5908
» https://doi.org/10.1200/JCO.2011.36.5908 -
34SEER Cancer Statistics Review, 1992-2012 [database on the Internet]. National Cancer Institute. In 2015. Available from: [http://seer.cancer.gov/statfacts/html/stomach.html].
» http://seer.cancer.gov/statfacts/html/stomach.html -
35Smalley SR, Benedetti JK, Haller DG, Hundahl SA, Estes NC, Ajani JA, Gunderson LL, Goldman B, Martenson JA, Jessup JM, Stemmermann GN, Blanke CD, Macdonald JS. Updated analysis of SWOG-directed intergroup study 0116: a phase III trial of adjuvant radiochemotherapy versus observation after curative gastric cancer resection. J Clin Oncol. 2012;30(19):2327-33.- doi: 10.1200/JCO.2011.36.7136
» https://doi.org/10.1200/JCO.2011.36.7136 -
36Songun I, Putter H, Kranenbarg EM, Sasako M, van de Velde CJ. Surgical treatment of gastric cancer: 15-year follow-up results of the randomised nationwide Dutch D1D2 trial. Lancet Oncol. 2010;11(5):439-49.- doi: 10.1016/S1470-2045(10)70070-X
» https://doi.org/10.1016/S1470-2045(10)70070-X -
37Stahl M, Walz MK, Stuschke M, Lehmann N, Meyer HJ, Riera-Knorrenschild J, Langer P, Engenhart-Cabillic R, Bitzer M, Königsrainer A, Budach W, Wilke H. Phase III comparison of preoperative chemotherapy compared with chemoradiotherapy in patients with locally advanced adenocarcinoma of the esophagogastric junction. J Clin Oncol. 2009;27(6):851-856.- doi: 10.1200/JCO.2008.17.0506
» https://doi.org/10.1200/JCO.2008.17.0506 -
38Tsuburaya A, Yoshida K, Kobayashi M, Yoshino S, Takahashi M, Takiguchi N, Tanabe K, Takahashi N, Imamura H, Tatsumoto N1, Hara A, Nishikawa K, Fukushima R, Nozaki I, Kojima H, Miyashita Y, Oba K, Buyse M, Morita S, Sakamoto J. Sequential paclitaxel followed by tegafur and uracil (UFT) or S-1 versus UFT or S-1 monotherapy as adjuvant chemotherapy for T4a/b gastric cancer (SAMIT): a phase 3 factorial randomised controlled trial. Lancet Oncol. 2014;15(8):886-893.- doi: 10.1016/S1470-2045(14)70025-7
» https://doi.org/10.1016/S1470-2045(14)70025-7 -
39Wang SY, Yeh CN, Lee HL, Liu YY, Chao TC, Hwang TL, Jan YY, Chen MF. Clinical impact of positive surgical margin status on gastric cancer patients undergoing gastrectomy. Ann Surg Oncol. 2009;16(10):2738-43. - doi: 10.1245/s10434-009-0616-0
» https://doi.org/10.1245/s10434-009-0616-0 -
40Xu J, Zhu J, Wei Q. Adjuvant radiochemotherapy versus chemotherapy alone for gastric cancer: Implications for target definition. J Cancer. 2019;10(2):458-466.- doi: 10.1245/s10434-009-0616-0
» https://doi.org/10.1245/s10434-009-0616-0 -
41Yakir R, Luna K, Marc W, Tamar S, Avraham R, Ayala H. The toxicity and outcomes of continuous 5-fluorouracil/cisplatin-based chemotherapy followed by chemoradiation in patients with resected high-risk gastric cancer: results of a single institute. Ann Acad Med Singapore. 2008;37(3):200-4.- PMID:18392298
-
42Ychou M, Boige V, Pignon J-P, Conroy T, Bouché O, Lebreton G, Ducourtieux M, Bedenne L, Fabre JM, Saint-Aubert B, Genève J, Lasser P, Rougier P. Perioperative chemotherapy compared with surgery alone for resectable gastroesophageal adenocarcinoma: an FNCLCC and FFCD multicenter phase III trial. J Clin Oncol. 2011;29(13):1715-1721.- doi: 10.1200/JCO.2010.33.0597
» https://doi.org/10.1200/JCO.2010.33.0597
-
Financial source:
none
Publication Dates
-
Publication in this collection
20 Dec 2019 -
Date of issue
2019
History
-
Received
01 July 2019 -
Accepted
17 Sept 2019

 Average=65.99; median= 60; SD=7.18
Average=65.99; median= 60; SD=7.18
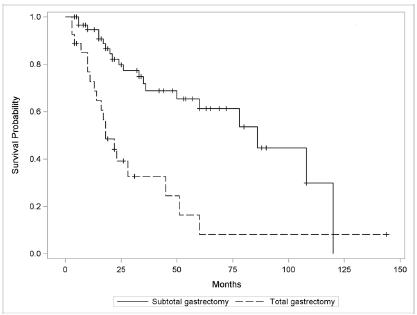 Subtotal - average=76.47; median=86; SD7.38. Total - average=27.34; median=18; SD=4.30
Subtotal - average=76.47; median=86; SD7.38. Total - average=27.34; median=18; SD=4.30
 Complete - average=73.26; median=86; SD=8.46. Surgery only - average=38.58; median=24; SD=5.67
Complete - average=73.26; median=86; SD=8.46. Surgery only - average=38.58; median=24; SD=5.67
 Yes - average=63.59; median=60. No - average=31.73; median=17. Overall - average=54.63; median=35
Yes - average=63.59; median=60. No - average=31.73; median=17. Overall - average=54.63; median=35