Abstract
The notification of sexually transmitted diseases (STD) is a prime component of well-designed public health policy. However, peculiar aspects of STD must be taken into account for the correct management of surveillance activities. Here, we describe the distribution of the most common sexually transmitted diseases among patients attended by the gynecological clinics of the principal public hospitals of Brasilia and the Federal District, Brazilian capital, during six years. A total of 142,158 patients had their cervicovaginal samples collected for Papanicolaou preparations and eventual biopsies. Diagnosis was made according to cytological and histological alterations, distinguishing among vaginal infections, and pre-cancerous and cancerous cervical lesions. We also looked at the annual prevalence of the various types of infections and alterations. There was a high prevalence of bacterial vaginosis, trichomoniasis and candidiasis, with suggestive changes over the years. Pre-cancerous and cancerous lesions increased 2.2 fold during the six years. A large proportion of the cases involved late stages of cervical cancer, indicating the necessity of prompt attendance of the population in a routine gynecological prevention program.
Sexually transmitted diseases; STD notification; STD epidemiology
A six-year follow-up survey of sexually transmitted diseases in Brasilia, the capital of Brazil
Augusto Simões-Barbosa; Gilvânia Coutinho Feijó; Joaquim Xavier da Silva; Isabel Irene Rama Leal and Tânia Wanderley Paes Barbosa
Catholic University of Brasília
Regional Hospital of Asa Norte, Brasília, DF, Brazil
Address to correspondence Address to correspondence Dr. Augusto Simões-Barbosa Universidade Católica de Brasília, DF; Campus II - Pós-graduação em Biotecnologia Genômica, SGAN 916, módulo B, Asa Norte Zip Code: 70790-160. Brasília DF Brasil Phone: 61 340 5550 (r. 154). Fax: 61 347 4797 E-mail: sbarbosa@ucb.br
ABSTRACT
The notification of sexually transmitted diseases (STD) is a prime component of well-designed public health policy. However, peculiar aspects of STD must be taken into account for the correct management of surveillance activities. Here, we describe the distribution of the most common sexually transmitted diseases among patients attended by the gynecological clinics of the principal public hospitals of Brasilia and the Federal District, Brazilian capital, during six years. A total of 142,158 patients had their cervicovaginal samples collected for Papanicolaou preparations and eventual biopsies. Diagnosis was made according to cytological and histological alterations, distinguishing among vaginal infections, and pre-cancerous and cancerous cervical lesions. We also looked at the annual prevalence of the various types of infections and alterations. There was a high prevalence of bacterial vaginosis, trichomoniasis and candidiasis, with suggestive changes over the years. Pre-cancerous and cancerous lesions increased 2.2 fold during the six years. A large proportion of the cases involved late stages of cervical cancer, indicating the necessity of prompt attendance of the population in a routine gynecological prevention program.
Key Words: Sexually transmitted diseases, STD notification, STD epidemiology.
Sexually transmitted disease (STD) management became a priority throughout the world due to the 1980's HIV pandemy. Notification of STD is a necessary first step for policy development. There are several aspects that should be taken into account for the designing of an efficient management approach. This includes surveillance findings of STD in the population and the determination of disease-risk factors.
In this scenario, one must be concerned about cultural and socioeconomic aspects of the epidemiology of STD. Obviously, sexual behavior is essential for STD establishment. It is clear that promiscuity and the non-use of condoms increase the risk of acquisition of STD [1, 2]. In addition, Brazil is a developing country that possesses profound socioeconomic disparities. Poverty, together with a low average educational level, result in increased SDT incidence. Thus, to have an impact, prevention policies must include substantial social transformations [3, 4].
Clinical management and prevention of STD are important aspects of public health planning since STD ranks among the top causes of disability-adjusted life-years lost in heavily affected urban populations [5]. Besides disease sequels, STD increase the risk of HIV infection/transmission and cervical cancer development [6, 7]. On one hand, ulcerative diseases are the strongest risk for HIV infection [8], while vaginal and urethral discharges are also important since they usually provoke large-scale recruitment of susceptible inflammatory cells [9]. Thus, a strong direct correlation with HIV infection is also found for intensive bacterial vaginosis, trichomoniasis, and others [7, 10, 11]. The correct treatment of infected populations could give two epidemiological results: i. it diminishes the spread of HIV infection; ii. it reduces the shedding of HIV infected cells [12, 13]. Certain types of Human Papillomavirus (HPV), mostly types 16 and 18, are recognized as human carcinogens. HPV is not necessarily a central cause but it is a necessary cause. Greater than 99% of cervical cancers contain HPV DNA [14]. In addition, epidemiological and experimental data strongly support the etiological role of HPV infection in the development of cervical cancer [15, 16]. Thus, it is assumed that effective prevention of STD leads to a dramatic reduction in cervical cancer incidence and mortality.
STD management is critical, but diagnosis is still controversial. STD diagnosis has usually been based on laboratory procedures. The accuracy of pap-smears is dependent on cytological experts and it could be inadequate for some types of STD [17]. Some improvements have been made, such as the development of very sensible molecular techniques, based on the detection of pathogen DNA [18, 19]. Unfortunately, this biotechnological approach may be inviable economically. In developing countries, simple laboratory procedures that involve trained observers and microscopes would normally be available.
We must be aware of local conditions in order to achieve efficient STD management. Mass treatment and syndromic approaches are some of the alternatives for intervention. Both of them are being investigated in terms of epidemiological results, but few data are available to determine if they have a positive impact on the STD situation. Symptoms do not always make vaginal infections distinguishable. The poor performance of the algorithm for managing vaginal discharge information limits the effectiveness of a syndromic approach [20, 21]. Moreover, asymptomatic patients are not benefited and unspecific symptomatic groups could be overtreated [22]. Consequent drug pressure could favor antibiotic resistant strains. This is a current epidemiological aspect that is a serious problem for disease management [18]. At this time, a multiple strategy must be taken into account for STD control: routine prevention, etiology (laboratory based), as well as syndromic, presumptive and immediate treatment. These three strategies depend on large investments in: i. Education, promoting prevention by appropriate individual sexual behavior and hygiene; ii. Public Health, providing primary health care; iii. Research, providing mechanisms for rapid, differential and accurate diagnosis.
We examined 142,158 female patients in a primary health care service for the detection of ulcerative and non-ulcerative vaginal infections, and the prevention of cervical-uterus cancer. Infections were notified and cytological alterations classified based on morphological criteria. This profile of the STD situation in Brasilia, the capital of Brazil, will help us evaluate STD management and prevention programs, and permit us to examine epidemiological aspects of our population, so that viable policies for STD and cancer control can be developed.
Methodology
Primary health attendance in northern Brasilia and the Federal District, the capital of Brazil, is composed of nine health centers. We collected vaginal and cervical samples from 142,158 women, who were attended by all the primary health-care centers in northern Brasilia and the Federal District. Samples were taken to the main hospital of Brasilia, HRAN (Hospital Regional da Asa Norte), where they were analyzed. Cervicovaginal smears were immediately mounted onto slides and fixed by immersing in 90% ethanol, taking care not to allow the smears to dry before they were fixed. They were prepared by the Papanicolaou technique, utilizing the three dyes: Harris's hematoxilin, Orange G and EA 65, as described elsewhere [23].
Inflammatory and non-inflammatory lesions were investigated based on cytological and histological microscopic exams of vaginal, exo- and endocervical smears and some biopsies. Malignant alterations were characterized according to typical cytological and histological criteria. Cellular and nuclear atypies were carefully analyzed for the correct identification of cervical neoplasias among the unspecific or normal tissue repair and cellular differentiation processes of hyperplasia and metaplasia. To accomplish this, we investigated irregular shapes, sizes and color of nuclei and the cytoplasm, koilocytosis, nuclear hyperchromasia with irregular distribution of chromatin and evident nucleolus, and intensive and abnormal mitosis [23]. Pre-cancerous lesions were identified as NCI (Neoplasia of the Cervical Intra-epithelium) categories I, II and III [24]. Cancer lesions become invasive whenever tumor cells infiltrate through the basal lamina [23].
The quality of the vaginal and cervical harvest was further verified, by looking for cylindrical endocervical cells, along with cervicovaginal epitheliam cells and mucus (Mitchel & Medley, 1992, 1993; Metcalf, 1994; Sidawy, 1993). By excluding unsatisfactory preparations and normal results, these exams can distinguish pathological inflammatory and non-inflammatory alterations, such as: NCI, invasive tumor, HPV, HSV, Candida sp, Trichomonas vaginalis, Chlamydia trachomatis, Gardnerella vaginalis, coccus, coccus/bacillus and unspecific. In this last category, an inflammatory lesion is characterized but not the etiological agent. Our data was organized according to individual prevalence of lesions or etiologies over the six-year notification period.
Results
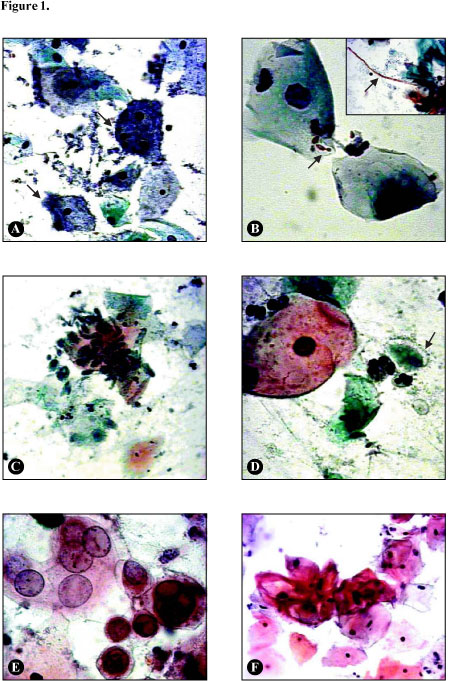
The Papanicolaou technique provides a clear distinction among several types of inflammatory lesions (Figure 1). As we could see, Gardnerella vaginalis, the most common cause, worldwide, of bacterial vaginosis, is characterized by numerous bacilli, partially or totally adhered to the surface of the epithelial cells, which become light blue. These bacteria-covered cells are named clue cells (Figure 1A). Candida albicans is detected in spore and filamentous forms. The dark yeast filaments get entangled while the brown darken spores possess a light colored, well-limited membrane; both features were used to define candidiasis (Figure 1B).
A marked inflammation is usually seen in trichomonosis. The protozoa Trichomonas vaginalis appears rounded or elliptical in shape, being 6 to 12 times shorter than the epithelial cells in the external epithelium. This parasite is also found adhered to these cells. It stains faint blue or gray and the peripheral nucleus strongly indicates T. vaginalis infection (Figures 1C and 1D). Chlamydia trachomatis is an obligate intracellular bacterium, found as eosinophilic vacuolar inclusions, preferentially in metaplasic cervicovaginal cells (data not shown).
Genital Herpes Virus (HSV) induces typical cytological alterations of the host cells. The nucleus appears larger in size and is limited by a well-defined membrane. Infected cells usually possess closely placed or overlaid multiple nuclei, which have a glassy aspect and contain eosinophilic inclusions (Figure 1E). Correct diagnosis of Human Papilloma virus (HPV) infection could lead to a better prognosis in terms of cervical cancer prevention. HPV infected cells develop nuclear atypies. Koilocytosis is predominant. It resembles neoplastic cells in which an enlarged nucleus is surrounded by a bright and clear cytoplasmic halo (Figure 1F).
The results from 142,158 Pap-smear cytological preparations during the six-year notification period (Figure 2) revealed a predominance of inflammatory lesions (65%) over negative results (34%) and pre-cancerous and cancerous lesions (<1%). The results were unsatisfactory, based on the criteria of the presence of cylindrical endocervical cells and cervicovaginal epithelial cells and mucus [25-28]. The absence of endocervical cells, few cervicovaginal cells, a large quantity of mucus, semen, and erythrocytes could mask the results. Unsatisfactory results were attributed to low-quality pap-smears, due to manual error, menstrual periods, and recent sexual relations. The prevalence of pre-cancerous and cancerous lesions affected the degree of neoplastic progression (Figure 3). Only 6% of the lesions were diagnosed early (NIC I). A large number of cancerous lesions were in an invasive stage (25%). This means that our population needs to be educated about cervical cancer prevention.
In our investigation of the etiology of vaginal inflammatory lesions, we found that in 31,143 cases (21% of the inflammatory lesions) the etiological agent could not be identified (Figure 4). Very intense inflammatory processes, added to the limitations of the Papanicolaou technique, could explain this fact. On the other hand, 22,536 cases among all results of infections (22%) were identified as coccus or coccus/bacillus infections (Figure 4). For a clear definition of most cases of bacterial infection it is necessary to make cultures. Despite this intrinsic limitation of our study, we found a predominance of infection with Gardnerella vaginalis (17.2%) over candidiasis (9.4%) and trichomoniasis (7.3%). However, bacterial vaginosis is not well defined as a sexually transmitted disease [29].
There was a 2.2 fold increase in the annual prevalence of pre-cancerous and cancerous cervical lesions during the six years of this survey (Figure 5A). As many of the lesions indicated a late stage in cancer progression (Figure 3), we again emphasize the importance of early prevention and treatment of cervical cancer of this population. The prevalence of HPV infection fluctuated over the years and did not follow the increase in pre-cancerous and cancerous lesions (Figure 5B). A slight increase in Gardnerella vaginalis prevalence (1.25 fold) occurred, while there was a slight decrease in candidiasis and trichomoniasis, 1.19 fold and 1.66 fold, respectively (Figure 5C, D and E). These numbers could reflect a normal variation in prevalence over the years, but it could also indicate a change in individual habits related to better prevention. Since bacterial vaginosis has other means of transmission, its prevalence could be maintained or could even become higher in comparison with others that are restricted to sexual transmission, such as trichomoniasis.
Discussion
It is apparent that STD prevention and clinical management has become a priority in worldwide public health policies. STD management is an important component of HIV prevention [30]. This is not a simple task. The distribution of STD has been found to vary widely [22]. Thus, an important first step for developing correct policy is to describe the distribution of STD and to search for epidemiological factors in the population under study.
During six years, we have followed the notification of STD in Brasilia, the capital of Brazil, based on cytological and histological criteria of cervicovaginal Pap-smears and eventual biopsies. We found a prevalence of bacterial vaginosis, comprising 33% of all cases. Our results confirm previous reports for other populations [22, 29, 31]. Although bacterial vaginosis is related to sexual behavior, it is not considered a classic STD [29]. During the six years, we observed a slight increase in the prevalence of the main etiological agent of bacterial vaginosis, Gardnerella vaginalis. This was accompanied by a small reduction in the prevalence of trichomoniasis and candidiasis. One reason may be that, in contrast to bacterial vaginosis, trichomoniasis is a classic STD, invoking specific types of control methods.
Although our data show few cases (3.6 cases per 1000), the 2.2 fold increase in the prevalence of pre-cancerous and cancerous lesions is alarming. In addition, most of the cases were detected at late stages; 55% were NIC III, or invasive cancer. This signifies a bad prognosis for the patient if not immediately treated. The fluctuation of HPV prevalence did not coincide with increases in pre-cancerous and cancerous lesion prevalence. We could not find a strict association between them, perhaps because HPV can be incubated during several years and only a few types of the virus induce cervical cancer.
Finally, our data suggest that the population of this study is not being regularly attended by routine gynecological disease prevention programs. Therefore, we should alert the community about STD prevention and induce political decisions. The next step, which includes an investigation of specific epidemiological aspects, should lead to a better program of STD management and control in our population.
Acknowledgments
We thank Dr. Martinho Gonçalves da Costa of the Hospital Regional da Asa Norte, through whose help we had the full collaboration of that institution. We also thank the Universidade Católica de Brasília for financial support.
Received on 15 January 2002
Revised 28 May 2002
- 1. Lignani Jr L., Oliveira E.L., Carneiro M., et al. Sexually Transmitted Diseases in Homosexual and Bisexual Males from a Cohort of Human Immunodeficiency Virus Negative Volunteers (Project Horizonte), Belo Horizonte, Brazil. Mem Inst Oswaldo Cruz 2000;95(6):783-5.
- 2. Eisenberg B. The Number of Partners and the Probability of HIV Infection. Statistics in Medicine 1989;8:83-92.
- 3. Parker R., Camargo Jr K.R. Poverty and HIV/AIDS: anthropological and sociological aspects. Cad Saúde Pública 2000;16(Suppl.1):89-102.
- 4. Csillag C. Sex education is key to combating AIDS in Brazil. The Lancet 1999;353:2221.
- 5. Mayaud P., Uledi E., Cornellisen J., et al. Risk scores to detect cervical infections in urban antenatal clinic attenders in Mwanza, Tanzania. Sex Trans Inf 1998;74(Suppl.1):S139-46.
- 6. Wasserheit J.N. Epidemiological synergy: interrelationships between human imunodeficiency virus infection and other sexually transmitted diseases. STD 1992;19:61-77.
- 7. Laga M., Manoka A., Kivuvu M., et al. Non-ulcerative sexually transmitted disease treatment as risk factors for HIV-1 transmission in women: results from a cohort study. AIDS 1993;7:95-102.
- 8. Schechter M., Marangoni D.V. Doenças infecciosas: Conduta diagnóstica e terapêutica. Guanabara Koogan, Rio de Janeiro, 1998
- 9. Laga M., Nzila N., Goeman J. The interrelationship of sexually transmitted diseases and HIV infection: implications for the control of both epidemics in Africa. AIDS 1991;5(Suppl. 1): S55-S63.
- 10. Sewankambo N., Gray R.H., Wawer M.J., et al. HIV-1 infection associated with abnormal flora morphology and bacterial vaginosis. Lancet 1997;350:546-50.
- 11. Cameron D.W., Padian N.S. Sexual transmission of HIV and the epidemiology of other sexually transmitted diseases. AIDS 1990;4(Suppl. 1):S99-S103.
- 12. Cohen M.S., Hoffman I.F., Royce R.A., et al. Reduction of concentration of HIV-1 after treatment of urethritis: implications for prevention of sexual transmission of HIV-1. Lancet 1997;349:1868-73.
- 13. Dallabeta G., Diomi C. Treating sexually transmitted diseases to control HIV transmission. Curr Opin Infect Dis 1997;10:22-5.
- 14. Walboomers J.M., Jacobs M.V., Manos M.M. et al. Human Papillomavirus is necessary cause of invasive cervical cancer worldwide (see comments). J Pathol 1999;189:12-9.
- 15. IARC, I.A.f.R.o.C. Human papillomaviruses. WHO 1995:277-82.
- 16. Muñoz N. Human papillomavirus and cancer: the epidemiological evidence. J Clin Virol 2000;19:1-5.
- 17. Amaral E., Oliveira U.M., Tambascia M., et al. A citologia oncótica na triagem das infecções cérvico-vaginais. In: Program and abstracts: XI Latin American Congress on Sexually Transmitted Diseases and V Pan-American Conference on AIDS, PO89, Lima: Peru, 1997
- 18. Carne C. Sexually transmitted infections. BMJ 1998;317:129-32.
- 19. Persing D.H., Smith T.F., Tenover F.C., et al. Diagnostic Molecular Microbiology, principles and applications. Rochester, MN: Mayo Foudation, 1993
- 20. Moherdaui F., Vuylsteke B., Siqueira L.F., et al. Validation of national algorithms for the diagnosis of sexually transmitted diseases in Brazil: results from a multicentre study. Sex Transm Inf 1998;74(Suppl. 1):S38-S43.
- 21. Brabin L. Clinical management and prevention of sexually transmitted diseases: a review focusing on women. Acta Tropica 2000;75:53-70.
- 22. Amaral E. Current approach to STD management in women. Int J Gynecol Obst 1998; 63(Suppl.1):S183-S9.
- 23. Gompel C., Koss L.G. Citologia ginecológica e suas bases anatomoclínicas. São Paulo, Brasil: Editora Manole Ltda, 1997
- 24. Richart R.M. The natural history of cervical intraepithelial neoplasia. Clin Obstet Gynecol 1967;10:748-84.
- 25. Mitchel H., Medley G. Influence of endocervical status on cytological prediction of cervical intraepithelial neoplasia. Acta Cytol 1992;36:875-80.
- 26. Mitchel H., Medley G. Cellular differences between true negative and false negative Papanicolaou smears. Cytopathology 1993;4:285-90.
- 27. Metcalf K.S., Sutton J., Moloney M.D., et al. Which cervical sampler? A comparison of four methods. Cytopathology 1994;5:219-25.
- 28. Sidawy M.K., Tabbara S.O. Reactive change and atypical squamous cells of undetermined significance in Papanicolaou smears: a cytohistologic correlation. Diagn Cytopathol 1993;9(4):423-7.
- 29. Nogueira R.C.M., Gomes F., Moro S. Vigilância aprimorada das DST em serviços que atendem pacientes com DST no município de Santos. In: Program and abstracts: XI Latin American Congress on Sexually Transmitted Diseases and V Pan-American Conference on AIDS, PCJ150, Lima: Peru, 1997
-
30Advisory Committee of HIV and STD Prevention. HIV prevention through early detection and treatment of other sexually transmitted diseases – United States. Recommendations of the advisory Committe of HIV and STD prevention 47, Morbity and Mortality Weekly Report, no. RR-12, 1998
- 31. Wawer M.J., Sewankambo N.K., Gray R.H., et al. Community-based trial of mass treatment for HIV control, Rakai, Uganda: preliminary data on STD declines. In: Program and abstracts: XI International Conference on AIDS, no. Mo.C.443 Vancouver: Canada, 1996
Publication Dates
-
Publication in this collection
06 Mar 2003 -
Date of issue
June 2002
History
-
Accepted
28 May 2002 -
Received
15 Jan 2002